When I was on the camel, I got a bit upset… I was sitting there on the camel. My dad wasn’t there to tell him. It’s the first holiday I’ve been on that he wasn’t there for me to go and tell him.
I am having a Cuppa Tea with Richard. We are recording our conversation for a brand-new podcast, a series of lovely 15 minutes episodes where my colleague Richard Keagan-Bull has a chat with someone about “things that matter to me”. I am the first lucky podcast guest.
That first episode was launched two weeks ago, when I was on leave from work. During the last few minutes of our chat, we contemplate what it’s like for us to have a job that needs us to think about death and dying. Richard (whose dad died last year) tells me what happened on his looked-forward-to camel ride during a recent holiday in Morocco.
I was on leave from work for the saddest of reasons. My sister had just died. I’d had a highly emotional week of hearing this devastating news, crossing the Channel and organising the funeral. They don’t hang about in the Netherlands. My sister was buried a week after she died. “Distressed” is an understatement. I was exhausted.
It was so exciting to produce the podcast together. I had been looking forward to the launch, but when I received an apologetic WhatsApp message from my colleague that my Cuppa Tea with Richard was now online (“Sorry to disturb you but I just wanted to let you know…”), I’d forgotten all about it. I was sitting in the French countryside (a planned and well-timed holiday) and decided to have a listen, as a distraction from my overwhelming grief.
Most of the podcast is about my journey from young nurse in the Netherlands to professor in the UK. I’d forgotten about that camel story at the very end of the 15 minutes. It hit me in the solar plexus.
Because that very morning, I’d had my very own Camel Moment. I had visited a French market and popped into a shop for some Retail Therapy, buying a top that I really didn’t need. My sister and I had our own word for this: Truitje Kopen, literally: Buying a Top. It was an expression we used for when you need some comfort or distraction from a distressing situation. I hadn’t realised that’s what I was doing, until I found myself in tears in the changing room. Because there is only one person to whom I could say: Look what I’m doing! Truitje kopen! and we would laugh together, and she’d understand. But she is dead.
It echoed an identical situation I shared with my sister exactly 10 years ago, when our mother was dying, and we went Truitje kopen together in anticipation of her funeral (complicated by my impending mastectomy in the very same week). I wrote a whole blog about it then, how I dissolved in a sorry flood of tears in the changing room. I called it Sudden Collapses in Public Places. How you can suddenly, unexpectedly and overwhelmingly, be hit by a wave of grief.
My Sudden Collapse in France was due to the realisation that I can no longer tell my sister about things, because I no longer have my sister. That’s specifically what Richard was talking about. His Sudden Collapse on a camel, because he no longer has his dad.
It will happen again, to me, to you. But now, thanks to Richard, we will have a word for it. If I’m floored again by a sudden wave of grief or tears, I can make sense of it and explain it very simply.
Don’t worry folks. I’m just having a Camel Moment!
A couple of months ago, one of my colleagues spotted that there was an “Employer of People with a Disability” category at the National Learning Disabilities and Autism Awards. How about nominating Kingston University?
YES! said Richard. We’ll nominate you! He sat down with Tasha, one of our team members employed specifically to support him in his researcher job, and told her what to write. They also added some of the contributions of his other colleagues. This is what they sent in:
OUR NAME IS ON THE DOOR, NEXT TO THE PROFESSOR’S NAME!
We are 4 researchers with a learning disability. Kingston University has employed us as proper members of the learning disability research team. They made it possible for us. They ran a research course. The application form was in Easy Read. Even our appraisals are in Easy Read. They employ support researchers to help us. They help us book taxis to get to work.
RICHARD: “We have the learning disability, we live it, we’re the experts. We’re more than just a pat on the back and we bring so much to this job. Working here makes me feel good about myself wearing smart clothes, going off to do a day’s work, getting paid for it. I feel valued. I can now shop in places I never used to be able to. This job has opened doors for me. I get to meet different people like professors and training the nurses of the future. I feel part of society.”
LEON: “I didn’t know you could be a university researcher, so I’m really surprised and pleased. It’s a warm, relaxed, friendly atmosphere. At lunchtime we all sit together, as equals, sharing our news.”
AMANDA: “We can do anything we want to do in our lives if we have the right support. But not everybody will think of employing someone with a learning disability. Now other universities can see, LOOK! These people can work together as a team. Why can’t WE employ someone with a learning disability?”
Only 5% of people with a learning disability have paid work. Kingston University is a trail blazer by employing us. What we really like here is that people look up to us, not down at us. They treat us with respect. We feel proud working here.
We were shortlisted. I was interviewed on Zoom. Thankfully, Richard and Amanda were in the office that day, so they could help me out – and they did. The judges said they were moved to tears by what they said, and by the short video we showed them.
Tears are promising, we thought. Might we win? But then again, there were 11 other organisations nominated in our category.
In any case, a good enough excuse to travel up to Birmingham with the entire team (except the three colleagues who couldn’t make it – one was at a conference in Australia, one was at home with her newborn baby, and one – David, one of our KEY researchers – was sadly unwell in Awards Week and missed out).
A gala dinner. The best way to explain what to expect was Imagine the Oscars. We talked about outfits. Several colleagues headed for the shops. For some, a black tie event was a lifetime first for which their existing wardrobe was unprepared.
How did you feel in the Posh-Section-Of-The-Shop? I asked. Like a VIP, was the answer of someone who still couldn’t quite believe that “VIP” and “me” belong in the same sentence.
The trip was worth it for this experience alone. Shouldn’t we all have moments when we feel like a Very Important Person? Because we are. We all are. So here is our group of 10 VIPs at our hotel just before the event, gasping at seeing each other all dressed up and ready to roll.
We felt like film stars… James Bond was invoked.
So, we had a great time. There was definitely GALA in the dinner, the stage was set, the music was ear-splitting, the food was fancy and spirits were high. And when KINGSTON UNIVERSITY was announced as winner, the cheers were loud.
I was a bit concerned about accessibility – for Disability & Autism awards, the event was remarkably autism-unfriendly, with its loud music and flashy lights; and the only way to the stage was with steps. I beckoned the presenter to come down, but Amanda was determined – nobody was going to stop her from going up. More confident of winning than I was, she had already rehearsed a speech. She took hold of the microphone, leaving the presenter with no option but to wave to the control room to turn the music down.
“I want to thank Kingston University for employing people with a learning disability. WE CAN BE RESEARCHERS!”
If that wasn’t enough to make everyone sit up, Richard then asked for the microphone and gave us one of the most memorable moments of the evening.
“Two weeks ago, my Dad died. He would have been so proud to see me standing here. When I was born, he was told that I would never do anything. And here I am now.”
I couldn’t be prouder of my amazing and utterly diverse team of researchers. It is just so very obvious that I need ALL of them. Going up to collect this award without my disabled colleagues would have been ridiculous.
Getting to this point has taken years of hard work, through setting up the GRASSroots group, through involving people as advisors in end-of-life projects, through writing papers together, through preparing potential researchers with learning disabilities with a training course, through working around the employment red tape courtesy of a willing HR team, and through time-consuming processes of finding funding not only for the disabled researchers, but also for the support researchers needed to enable them to contribute to their fullest. The time and resources needed to do this kind of inclusive research cannot be under-estimated. But oh, it is worth it.
It isn’t all plain sailing. Research work is precarious and dependent on finding funders interested enough to invest in our Cinderella topics. (Death. Learning disability.) Few researchers are on permanent contracts. In my team of 11 people, I am the only employee with a permanent position – everyone else is dependent on external research grant funding, with their jobs ending when their project ends, unless I find new project grants – not easy when I’m busy running my current projects.
So, my hope is that Richard, Amanda, Leon and David are able to show how indispensable they are, not only as part of our research team but also as trainers of future generations of health and social care staff. Perhaps it’s time to offer people with a learning disability a permanent position, not just at learning disability research faculties but also at university schools of nursing/social work/etc.
If TEAM BUILDING was part of the reason for getting all of us to Birmingham (quite a feat of organisation, let alone the expense – Gala Dinners come at a cost that won’t be easy for nominees on low budgets, so THANK YOU to the Kingston School of Nursing for funding our table), then it’s Mission Accomplished. But it has also done something else – something rather unexpected, given that these were the LEARNING DISABILITY & AUTISM awards: It has made my colleagues think about the true meaning of inclusivity. They looked around and wondered: WHY aren’t there more people with a learning disability here? Why is the stage so inaccessible?
Why, after we were applauded on stage, did someone come up to Amanda and indulgently stroke her face, as if she was a pet rather than a person? I was too taken aback to say anything, but it made me remember all the other moments I have been with Amanda when strangers have stroked her hair or touched her face unexpectedly and without asking. So let me ask you: Have YOU ever been petted by a complete stranger? No? Thought so. Me neither. (Perhaps people with disabilities need their own #MeToo movement.)
Perhaps this is a low note to end on… We really are delighted with our win, but we are also aware that we all still have a long way to travel. In the meantime, hats off to Kingston University for supporting us in thinking outside the box and cutting the red tape that enabled me to employ people with a learning disability as full (and fully paid) members of my team.
You work in the health service, or perhaps in social care. You get a referral for a man in his 70s. He has an intellectual disability and he is autistic. He feels he is suffering so much, he cannot bear it. His doctor explains to you that this is because:
As he has never been able to keep up with society, he has become insecure, with recurring depression. Due to his intellectual disability, he feels a great pressure of the world on him which he can not handle. His autistic traits make it increasingly difficult for him to cope with changes around him.
This reminds you of another man you support, much younger, just in his 20s. He, too, is suffering, because (and this is, again, his doctor speaking):
The patient has felt unhappy since childhood and was persistently bullied because he was just a bit different from others… He longs for social contacts but is unable to connect with others. This reinforces his sense of loneliness. The consequences of his autism are unbearable for him.
What can you do? What can we all do, as professionals, as families and friends, as policy makers, as funders, as a society?
There is no doubt that some people suffer deeply and profoundly, that the support they need is complex, and that you may well feel helpless, because some of the things that would really help are beyond your influence. Societies are not level playing fields. Too often, there is not enough understanding, not enough room for difference, not enough support.
What these men needed, it seems to me, is a society where they feel they belong, with people around them who not just accept and accommodate, but welcome their unique ways of being.
What this needs is a huge culture shift, but also a significant investment in highly individualised support services.
You feel helpless because cultures take a very long time to shift, you cannot magically find friends for these men, and your services are under-resourced. So what is the answer here?
I haven’t made these scenarios up. These were real men. They lived in the Netherlands. They asked for euthanasia. In the Netherlands, lots of people (around 1 in 20) die through euthanasia. If you are suffering unbearably, and there is no prospect of improvement, this is an option.
Their doctors agreed that euthanasia was the only acceptable option left for them, because (they explained) “Autism Spectrum Disorder is incurable”, and so is intellectual disability, so there really was no prospect of improvement.
These are just two stories out of 39 Dutch cases we analysed. Thirty-nine people who had an intellectual disability, or who were autistic (or both), and who died through euthanasia (a doctor giving a fatal injection at the patient’s request) or assisted suicide (the patient taking a fatal drug, with a doctor’s help). We looked at what caused these people to suffer. What made them ask for death, and on what grounds did doctors agree to their request?
We found that for the majority of people (two thirds of cases), it was factors associated with the intellectual disability or autism itself, which led to their suffering, their request to die, and the doctors saying yes. Factors like the ones described above: social isolation, loneliness, not being able to cope with life or with changes, being oversensitive to stimuli.
Our paper on this study has just been published. Here is a summary poster. At the bottom of this blog post, you can find our full paper and a 5 minute summary video (click on the images below). Please share these widely, because we need to continue the debate on assisted dying.
What are YOUR thoughts?
These are the questions I am asking myself:
If you agree to an assisted death for people who are suffering because of their autism or their intellectual disability, are you really saying that being autistic or disabled is HOPELESS? That is the word used to justify these assisted deaths: hopeless. No prospect of improvement. It seems to me that this places the problem within the person themselves. But is it the “patient” who needs to change or improve?
Or is it society? How can we build societies where people do not feel lonely or overwhelmed?
I wonder whether the option of an assisted death in these cases helps to build such a society – or hinders it.
It’s been a while since I’ve blogged here… We’ve been blogging away on our project website, but let me pick it up again and tell you about my work here. First of all, let me copy-and-paste a blog post I wrote a couple of months ago for the Victoria & Stuart Project, which brought back so many memories that I want to share it on this website too, in case you missed it.
Thinking about John
The year is 2006. I am a brand new researcher, sitting in the Research Advisory Group in the first year of my first major study into the needs of people with learning disabilities who are at the end of their lives. I am reading the group the story of John Davies, one of my first research participants.
John has been diagnosed with a devastatingly advanced form of penile cancer. He has ignored his symptoms for many months, and despite initial hopes to the contrary, both surgery and chemotherapy have proved insufficient to keep the cancer at bay. He is dying, and he knows it.
I explain to him that my job is to tell the stories of people like himself, and he is delighted, because telling his story is one way to make sense of it. He takes ownership, dictating the story of his life and his illness fluently into my little microphone. It is the draft of this story I am reading to my group of advisors, which includes a professor of learning disabilities, a hospice doctor, a psychiatrist, and two people with learning disabilities. As part of ongoing data analysis, I want to get their perspectives on it.
“Hello, my name is John Davies,” the story starts.
“I am 44 years old. I’ve got cancer, and I don’t want to happen to other people what happened to me. I left it far too late.”
John talks briefly of his childhood: “Name calling is the worst thing that happens, and it’s no picnic being called a spastic. But then I’ve learned to think, ‘sticks and stones break my bones’… and I just kept plodding along, going along in my own little way.”
He then quickly moves on to telling us how he became seriously ill, how he went to the doctor with pain when he went to the toilet but was sent home with antibiotics for a urine infection, and how he subsequently ignored worsening symptoms. First he thought it would clear up (the doctor had said so), but then he simply became too embarrassed to tell anyone. He explains:
“I really found it difficult when it got worse. I found it difficult to hide because by then it was noticeable not only to me (I could see it), but everybody else could smell it. There was a bad smell coming, and it didn’t matter how many times I got in the bath… My mum noticed that I was getting skinny. I said not to worry, that I was OK. But I wasn’t really OK at all. And I was very tired.
In the end I just went home and went to bed, and I didn’t get out for 4 days. My mum said to my brother: ‘You go round and see John, I am worried about him’. So my brother came round, pretending that he was just passing by and that he wanted a cup of tea. Well, if he wanted a cup of tea he wouldn’t have got one because I had the tea bags but no milk: I hadn’t been out of bed for 4 days. I just had bottles of water beside me to drink from, and I was using a bucket to do wee-wee. There was nothing coming out the other end because I weren’t eating anything. I’d let it get untidy and there was a bad smell because I couldn’t empty the bucket that had the wee-wee in. I hadn’t been able to keep the house clean, everything that was in the house smelled of wee-wee. Later on the council had to come and fumigate the whole house.
When my brother came he just took one look at me. I tied the coat round me but the coat fell off and he saw this lump, and this stuff coming out of it… It made him feel sick. He just got on the phone and called the ambulance there and then. And I got carted off to hospital.”
The story continues with treatments, in and out of hospital, hopes raised, hopes dashed, and worst of all: having to tell his mother that he has cancer.
He concludes:
“Sometimes I think: I wish… But you could wish a thousand wishes, and there is nobody with a magic wand to make it better. Sometimes I look at myself and think, ‘I lost my dingly-danglies. And I could have saved them. Now I take one day at a time. Life is too short, so I take one day at a time. You try to make the best out of a bad thing, which is what I have been trying to do.”
I manage to get to the end of reading the story, just about.
But by now, several people in the meeting are so distressed that we stop, make some more tea, and talk about it. The doctors and nurses in the group are devastated by the terrible sequence of events, from first mis-diagnosed symptoms to the final verdict that the cancer has come back and John will die. But our two advisors with learning disabilities are particularly upset. They are crying. What has upset them most? There was barely anything in John’s story that was not upsetting.
But what they focused on was the one thing I had glossed over, one thing I had not picked up as important.
“He was bullied at school,” one advisor says. “That happened to me.”
The other advisor nods, in tears: “Yes, me too.”
That was my first lesson in the importance of having people with learning disabilities help us with making sense of what we hear in our research. They brought a perspective that turned out to be crucial. They helped me see that your life-long experience of not being important, not being valued, shapes the way you experience serious illness.
Yes, John was devastated by having such a terrible form of advanced cancer, but he was unexpectedly uplifted and delighted by all the attention he received in the hospice: “They treat me like a king”. And he could never have dreamed that anyone would ever want to read his story. I managed to get it published under his own name (we had to go back to the Research Ethics Committee to allow him to do this), and I showed him the proofs nine months after I first met him. He was amazed and delighted.
“I have achieved everything now,” he said.
He died a few days later. You can read his story here.
I have never forgotten John. He has stayed with me all these years.
He also became the posthumous model for the main character in the Books Beyond Words story Am I going to die? (We used those pictures a lot in our focus groups).
John Davies on stage, supported by St Christopher’s Hospice, a few weeks before he diedImage based on John Davies, taken from Am I Going To Die?
Nine people with learning disabilities are meeting in the All Together Group, to help us think about good ways to plan for the end of your life. We are experimenting with the “Washing Line” idea: telling the story of your life with pictures and other items pegged along a long line that symbolises your life. We wonder whether that might help us think about the remaining, still-empty bit of washing line: What would you want to see there?
Richard has agreed to try it out. We think we know his story already, as he published his a book about his life last year. It’s a brilliantly triumphant one of achievements against the odds. Richard starts his washing line as he starts his book, with him mum who was told to “put him away” along with his disabled brother, because they’d never achieve anything. We watch and smile and cheer as his line fills up with being a college student, a baker, a swimmer, an artist, an advocate, and eventually a university researcher. Someone who lives in his own flat and makes his own choices.
And yet, at the end of all this, when I am thinking about the marvellous way in which we can now all visualise and applaud Richard’s life (and applaud we did), and pondering how that might help planning for what comes next, there are tears in the group. Why?
Because Richard’s parents were told that he was not worth anything.
The person who cries about this (“That brought back memories because the same happened to me”) has others wiping their eyes. Me too, me too.
And once again I am stopped short. Here we are, busy trying to make sure people are valued at the end of their lives, trying to make sure they have their wishes met when they are dying. But perhaps we are not quite seeing the huge impact of being told, right from when you are first born, that you shouldn’t really have been alive in the first place. That your parents shouldn’t have any more children in case they have another one like you.
A lifelong message that is reinforced by bullying and abuse, discrimination, by the unspoken (perhaps no longer noticed) impact of nobody coming to sit next to you on the bus.
Making end of life choices? In advance? And people actually listening to your wishes?
Perhaps that possibility is as surprising, maybe even unimaginable, as it was for John to find himself treated like a King and see his name in print.
“Too many pages of Easy Read are boring and stressful. We won’t read them.”
That was the loud and clear message from the Staying Alive and Well group. They are my colleagues with a learning disability who help us with jargon-busting saying easy words.
There are seven people with a learning disability in the group. They looked at different examples of making complicated information easier to understand and then held a series of meetings to ask ten other people with a learning disability for their opinion.
Easy Read came third on the list of preferences, after ASKING SOMEONE TO EXPLAIN and VIDEOS.
Easy Read was developed for people with a learning disability to help them understand important information. It uses short sentences, easy words and pictures. If you’re new to this concept, you can google it or read more about it on this page from PhotoSymbols (we, along with many others, often use their brilliant pictures).
“Translating” important but complicated documents into Easy Read is definitely 200% better than having no easier-to-understand information at all. In fact, when a new and important document is published that concerns people with a learning disability, I tend to go to the Easy Read version first.
But how easy is Easy Read for people with a learning disability? Is it easy enough? Is there any way of making it even easier?
This is what our groups said, having looked at different types of Easy Read documents as well as other formats of accessible information (stories, picture books, videos):
Easy Read is OK. Some people really like it. They are used to it. They want to see more of it.
But it needs to be short – just a few pages. No more than five pages.
If it’s longer, split it into different parts, with colours. And please, could you also put the Easy Read information on a video.
We asked the question as part of a Finding Out More* mission: “What is the best way for you to find out more about diabetes?”
*We’ve dismissed DEEP DIVE as definitely not being easy
It made us think, not just about diabetes, but about everything we try to make easier to understand. So now we were faced with a serious challenge. Can we put our money where our mouth is?
The next task for the Staying Alive and Well group was to make the LeDeR 2021 Annual Reportaccessible. It definitely – DEFINITELY – ticks the box for being important to understand. It analyses what happened to 3,304 people with a learning disability who died in England in 2021. What did they die of? How old were they? Who was most at risk from what? Lots of questions, and crucially this one: How does that compare to people in the general population?
The full report is 93 pages long, and that’s not counting all the extra bits (“See Appendix” etc). It’s packed with complicated numbers, tables, pie charts, and complex explanations. But at the heart of it, there are people who lived, were loved, and died. That’s the awful part. We are talking about people, yet we have to look at numbers. It’s important to understand the implications of the numbers. The implications have stayed distressingly similar, year after year of LeDeR reports, so really, it is saying nothing new. Until the numbers change dramatically and the need for LeDeR is eliminated, we need to keep reporting and we need to keep making sure that is is easy to understand. (Are deaths ever easy to understand? Especially avoidable deaths?) However frustrating that change is slow, or you might say non-existent.
We were helped by the efforts of those who produced LeDeR’s Easy Read reports in previous years. They included a lot of detail, which was an advantage but also a disadvantage, as it took it the Easy Read documents to well over 40 pages. How on earth could we distill all this in the few Easy Read pages people said they preferred? We worried about leaving too much of the detail and nuance out of it. But in the end, we agreed that having a few pages that you might actually engage with is better than feeling so overwhelmed by the information that you don’t take any of it in.
This is the first year that the new Staying Alive and Well group had this job. I’m grateful to the group members, because thinking about so many people dying is not easy. Not ever. Especially if this could be about you. Especially if you recognised, among all those numbers, the stories of friends who had died. But they all came to the meetings and kept coming, because they insisted it was important. (And of course they were paid for their work on this report.)
This is what we did.
Step 1: Present the report in sections, with different colours.
There are six chapters in the main report. Having listened to the group, we turned these into six different colours. Initially, we numbered them as well – but we noticed that people got in a muddle when they read this out, so they asked to get rid of the numbers altogether:
The grey part: Who died, and how old were they?
The yellow part: What did people with a learning disability die of?
etc.
Step 2: Not too much detail.
You simply cannot explain more than the headline messages. That means that you have to figure out what your headline messages are. Helpfully, the big main report now has a page of key “Take Away” messages at the start of each chapter, but even that was sometimes too much information for our group. Here are two of the key “Take Away” messages from The Grey Part, which we all thought should definitely go into the Easy version:
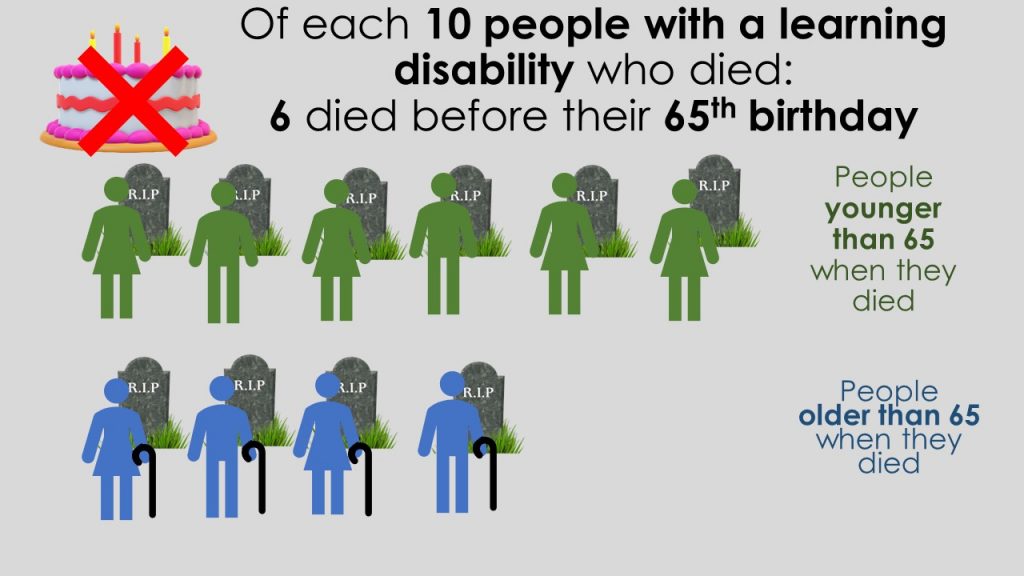
6 out of 10 people living with learning disability died before they were 65.
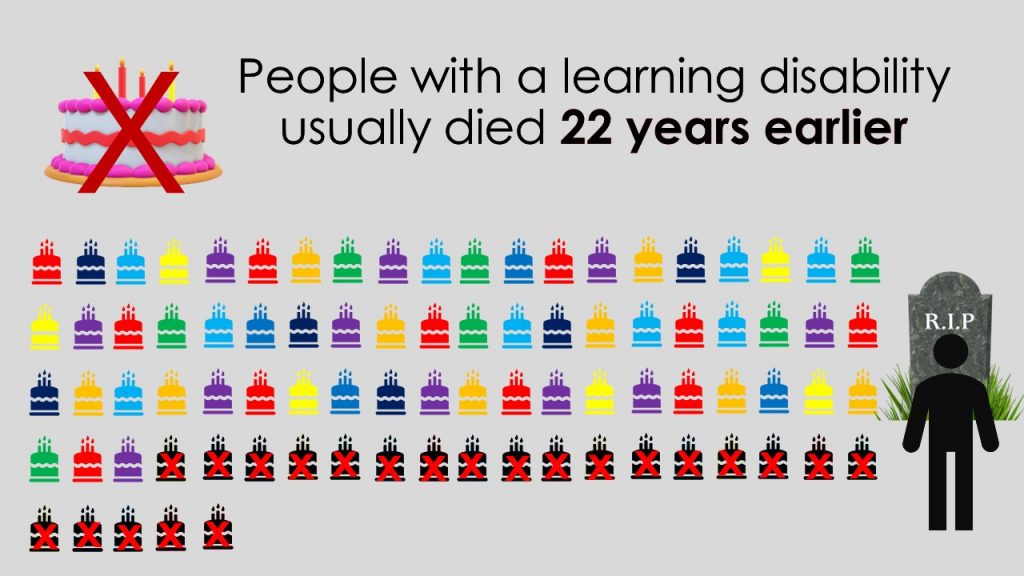
On average, males with a learning disability die 22 years younger than males from the general population, and females 26 years younger than females from the general population.**
But even in those key messages, there was too much information. We found that making things accessible involves taking things out. And then taking more things out. And more things. The hardest thing is deciding what to keep. So, we asked ourselves again and again: WHAT IS MOST IMPORTANT HERE?
Sometimes, on the other hand, we found that we had to put things in. Explain things. Put them into context. Why is it so important to know that only 40% of people make it past the age of 65? It’s because in the general population, it’s more like 85%.
**It’s so upsetting that these figures have barely changed… we get a similar headline year after year after year. Some people might see it as mildly positive that the average age of death for people with a learning disability is now 61 years, whilst in 2019 it was 60 years. But I am part of the much luckier “general population” and can expect to live well into my 80s, and all I can see – and my disabled colleagues with me – is the still too glaring gap of 22 years.
Step 3: Communicate your message in the easiest possible words
When we asked people what makes information easy to understand, they said “stories”. It’s probably true for all of us. Stories are so important, because they are about people, and people matter. It’s the awful stories of people who died too young, those that died avoidable deaths, that we remember and that should be the catalysts for change. Oliver McGowan. Richard Handley. Connor Sparrowhawk. They are just a few among so many, too many. Our group really understood the importance of their lives and deaths, and by implication, the lives and deaths of all the people in all the LeDeR annual reports.
But in this report, we were not talking about just one person, but about more than 3,000 people. There is an important place for the lessons we need to learn from each of their stories, but here, we were talking about averages and percentages. “Some people lived until they were 85, but many didn’t.” How to explain this?
We tried it in various ways and listened carefully to what people were able to explain back to us. What did they understand best? We ended up with this:
Of each 10 people with a learning disability who died, six died before their 65th birthday.
But of each 10 people who don’t have a learning disability, only one died before their 65th birthday.
People with a learning disability usually died 22 years earlier.
The group thought about each sentence, each word. Should it be 22 years younger? or 22 years earlier? It was time consuming but worth doing, because so many times, the group improved my own attempts.
Step 4: think about INFORMATION and EXPLANATION
Most of our accessible report is information.
What was good about people’s care?
Annual health checks helped people get good care.
Learning disability liaison nurses helped people get good care.
But there were times when we thought that extra EXPLANATION was needed – sometimes this wasn’t in the main report, so we had to add it:
They are special nurses who understand what people with a learning disability need.
Chapter 5 on Avoidable Mortality was the most difficult to explain. In fact most of that part of the Easy Read version (The orange part: Could more people with a learning disability have lived longer?) is explanation, different from the main report, and probably still not quite understandable enough. This is the main report’s “Take Away” finding:
49% of deaths were rated as “avoidable” for people with a learning disability. This compares to 22% for the general population.
But what exactly is an avoidable death? How to make sense of this? Trying to explain it, I realised I didn’t completely grasp the finer details myself. As always, trying to explain things in an easy way really throws up your own shortcomings in understanding. Initially, I could not make this chapter understandable, so I had to spend some time getting my head around it. I’m not sure we succeeded in making this complicated chapter truly accessible, but we tried to make a start. It is arguably the most important chapter of all.
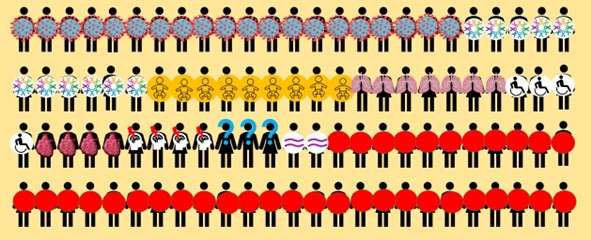
Step 5: Find images that REALLY explain what you are saying.
These are complicated concepts, so the words had to be supported by images that really helped to communicate the message. They should, ideally, be able to stand alone. We tested this by showing images before the words, and asking people to tell us what they thought the images were saying.
It was difficult, not least because death is so difficult and upsetting. Not making death clear was unhelpful, but was it too harsh to represent it clearly? There was no nice way of showing that over 3,000 people have died. The people in the group didn’t like the harshness of gravestones, for example, but then decided that taking away the gravestones made it less upsetting, it also made it less clear. In the end, they went for clarity.
We tried several ways of presenting the numbers. We don’t claim to have got it right. Different people understood different images. One person in the group really liked pie charts, but not everyone understood those. The group initially liked this pie chart draft, but it was rejected after we had to add more pie slices (the numbers are not quite right here, but with everything added in properly, it became even more confusing):We ended up with images like this:
Explaining 61% as “six out of ten people” was easier than the more accurate “sixty-one out of a hundred” or (as one external advisor would have preferred) the actual exact number out of 3,304. Here is our final approach to the “six out of ten” message:
But throughout our Easy Read report, you will see several different approaches. That’s because we found that repeating the same concept for different messages (e.g. ten people and their gravestones) was in danger of becoming not just confusing but “boring” and “stressfull”.
The strongest image ideas came from the group. How to show, without words, that on average people died 22 years earlier? One group member said, Well, they won’t have as many birthdays. So we could show birthday cakes and then cross them out.
In the video version (see Step 6) they thought we should make the cakes quite literally disappear. We played Happy birthday over it, stopping abruptly once it had counted down 22 cakes, with a gravestone appearing. I can’t say often enough how shocking this statistic is, and how shocking it is that it has changed so little since it was first reported in 2013. When we showed the video to non-disabled people, who (like me) had read these statistics year after year, they said that it really brought home the grim reality of it. We can know things, but sometimes we need the simplest of explanations to really understand them – and it is my learning disabled colleagues who were able to point out what the LeDeR findings mean to them, personally. We won’t have as may birthdays as you.
Step 6: Create not just a paper version, but also a video
Actually, our group insisted that the video should come first. The paper version of the LeDeR 2021 Easy Read Report looks quite different from what you may be used to. It’s two or three main picture-messages on a coloured page. That is mostly because we concentrated on the video, so the paper version is really a video-on-paper. We haven’t followed the standard credo of “picture on the left, sentence on the right”. I have no idea whether this is any good, so please tell us.
The video was made using PowerPoint slides with our group members reading the text, coping admirably with the jargon. Minority ethnic backgrounds. Avoidable. Reasonable adjustments.
We have thrown convention and rule books in the wind. Whilst this was based firmly on the views and contributions of our colleagues with a learning disability and feedback from their peers, it was only a handful out of thousands and thousands of people with a learning disability who they tried to represent. As an academic researcher, I’d much rather have tried and tested everything more carefully before releasing it into the world.
So we would really love you to give us feedback. You could be our testers. Tell us what you think and we will hopefully get better and better in making Easy Read truly Easy. We need to hear this, because we think we should do more. Whilst we could only include a few key messages, we would like to say a little bit more about each coloured part, perhaps in six separate, shorter videos.
And next year, I’m afraid we will have to do the same job again. We’d love the LeDeR programme to become redundant and unnecessary, because lessons have been learnt and acted upon. I’m hoping against hope that in next year’s video, we get to keep all the birthday cakes, but change is slow and I’m not holding my breath.
In the meantime, let’s all say THANK YOU to Richard, Frankie, Lee, Maggie, Amanda, Andrew and Joanne, and all those supporting them.
I love the way in which my colleagues and collaborators with learning disabilities help me to understand my job by simplifying the language. My colleague Richard leads the way in this. (If you haven’t met Richard, you can read about him here and here).
One of the delights of doing research with people with learning disabilities is also one of the greatest challenges. How to make sure we all know what we are talking about? For example…
Jargon alert #1 LeDeR: Learning from Lives and Deaths of People with a learning Disability and Autistic People
That’s the name of the project we started working on last autumn. It’s led by Kings College London who will do all the complicated things: looking at thousands of reports of deaths, doing the number crunching, figuring out whether (and crucially, why) people died before their time.
The job for Richard and myself (at Kingston University) is to lead the Co-Production Partnership (jargon alert #2! Co-Production Partnership? How about Working Together?). We set up a group of seven (so far) people with learning disabilities who meet once a month on Zoom.
It was clear at the first meeting that LeDeR was a confusing word that invited thoughts of Boris Johnson (no, we’re not talking about that kind of LeaDeR…) and was only understood after a fairly lengthy explanation. What to call this project then? We sat down in the office to ponder the matter. Richard knew the answer.
STAYING ALIVE!
Well, bingo. We threw Richard’s suggestion into the group, and into other groups (we happened to give a couple of talks during the following weeks). There was a unanimous thumbs-up. Finally, we knew what we were talking about! Preventing premature deaths – that does indeed mean Staying Alive.
We later decided to expand it to Staying Alive and Well, because this work isn’t just about stopping people dying too young: it’s about making sure that everyone lives a life that is as full and healthy as possible. So now we not only have a name that tells me what I’m supposed to be thinking about, but also a theme tune that sees us dancing on Zoom whenever our brains get too frazzled from thinking and talking.
We also have a logo, courtesy of a competition we launched for people with learning disabilities. The winning entry was judged solely by the group members with learning disabilities (I didn’t get a vote).
Jargon alert #3
Deep Dive
We’re now onto jargon alert #3. NHS England has asked us to do a couple of Deep Dives every year. It’s taken us months to come up with a good way of understanding what that means. My suggestion of Having A Closer Look was vetoed by the group, because are we really going to take a magnifying glass and actually look at something? We have settled on Finding Out More.
People with learning disabilities are the real jargon-busting experts. At our most recent Staying Alive group rmeeting, we spent a good couple of hours going over the easy-read report I’d written about the work they did for a Finding Out More question about diabetes. I was rather proud of the easy sentences I’d come up with, but quite a few of them were rejected and then improved by the group. My version…
TOP TIP: Make sure doctors and nurses know where to find accessible information.
The group’s improved version…
TOP TIP: Make sure doctors and nurses know where to find VIDEOS and EASY-READS about diabetes.
The joy that is emerging from the jargon busting (sorry: saying easy words) challenge is that it forces me to clarify (and thereby understand) what I’m actually talking about. Accessible information? What does that mean? THIS is what it means. We want videos and easy words.
Try it. I challenge you to try explaining your work to a complete novice in just one minute, using NO JARGON. For someone who needs easy-to-understand language, that might be all you’ve got, so you really need to understand what lies at the heart of your work. If you can do it, congratulations. If you’re struggling, join the club, and let’s keep working at it.
I am still struggling with this one…
Jargon alert #4
STAKEHOLDERS, anyone?
(or perhaps this was jargon alert #0, as it has been with me for years and I still haven’t managed to solve it, despite having asked many people with learning disabilities.)
In the meantime, Richard has found a jargon-free way to describe all three projects he is working on. There’s the Growing Older, Planning Ahead study we initially employed him for last year, looking at ways to support older people with learning disabilities who live at home with their families to plan ahead for the future. Then there’s our new study starting next month, on end-of-life care planning with people with learning disabilities.
So now, Richard will tell you, our week looks like this:
I’ll be Staying Alive on a Tuesday, Growing Older on a Wednesday, and Planning My Funeral on a Thursday.
Welcome to the world of a University Research Assistant.
You can follow us on twitter:
@AliveLeder (Staying Alive and Well)
@derwem (Richard Keagan-Bull)
@TuffreyWijne (me)
My quick answer to that is: If it is, then I have yet to hear about it. Let me explain.
Here’s a real-life (or rather, real-death) situation.
A woman in her 70s had stomach cancer. She had part of her stomach taken out, which quite probably cured her. But now she had to learn a new food routine – lots of small meals, rather than the three square meals a day she was used to.
She couldn’t cope with this. The woman was autistic and probably had an intellectual disability as well. She lived in the Netherlands and asked for euthanasia, which was granted. She died in 2020. The report on the Dutch Euthanasia Review Committee website explains why this fell within the legal euthanasia due care criteria of “intolerable suffering without prospect of improvement”:
The physician has clearly described why he was convinced that the patient’s suffering was hopeless and there was no other reasonable solution. The inability of the patient to cope with her new limitations stemmed from her Autism Spectrum Disorder, which was not treatable.(Case 2020-114)
This story is not unique.
I have blogged about this before. I am haunted by it. In 2017 and 2019, we published papers on our research into Dutch euthanasia cases that involved people with intellectual disability or autism (see here and here).
It’s my least favourite research topic, and yet it is arguably one of the most important, because the implications are so enormous.
It is probably these papers that led to a request for me to present evidence to the Quebec Select Committee on the Evolution of the Act respecting end-of-life care.
(This is a euphemism if ever there was one. Much along the lines of the Dying with Dignity Bill. I absolutely prefer the Dutch straightforward approach. Theirs is called the Termination of Life on Request and Assisted Suicide Act, which at least does at is says on the tin.)
However much I wish this topic would simply go away, I felt it was my duty to inform the Quebec Select Committee of the facts. If you are contemplating expanding assisted dying laws, then you need to know what the implications are for your most vulnerable citizens.
The wonders of Teams meant that I didn’t have to fly into Canada, but could talk to the Committee this afternoon from the comfort of my own home, with a translator speaking miraculously into my ear via headphones and a phone app.
It’s so important that I am publishing my full presentation to the Select Committee on my blog. It was followed by 40 minutes of questioning, which you can watch here if you understand French (as it’s dubbed), or on the video below without the dubbing (introduction and questions in French, but my presentation and my answers to questions in English).
Presentation to the Quebec Committee on the Evolution of the Act respecting end-of-life care
25th May 2021
Thank you very much for inviting me to present evidence to this Committee.
My name is Irene Tuffrey-Wijne. I am a professor of Intellectual Disability and Palliative Care at Kingston & St George’s University in London, UK.
In the next 20 minutes:
I am going to tell you who I am and what work I do;
I am going to define intellectual disability and autism;
and then I’m going to give you the evidence from my research as to what happens to people with intellectual disability or autism in a situation where the law has been changed to allow euthanasia for them.
But before I do that, I want to put before you these fundamental questions:
If there is a change in the law, where does your duty lie to make sure that the changed law is safer and better for your citizens than if there is no change in the law?
What is your duty of care to citizens who have a disability? What is your duty of support and suicide prevention, trying to improve their quality of life, and at what point do you abandon those efforts and offer them an assisted death?
My area of expertise
I speak to you today from my somewhat unique perspective as an expert in end of life care for people with intellectual disabilities or autism, and the world’s first professor in this subject. I would like to set out both the scope and the boundaries of my expertise. I am a nurse with extensive clinical experience in both intellectual disability and palliative care provision. For the past 20 years, I have conducted research into the experiences and needs of people with intellectual disabilities at the end of life.
With regards to the assisted dying debate, it is also important to point out that I am a citizen of the Netherlands and lived there until I moved to the UK in early adulthood. I have detailed research-based insight into both the laws and the practice of euthanasia in the Netherlands in relation to people with intellectual disabilities or autism, which I will draw upon for this presentation.
I am not in a position to comment on assisted dying legislation for people with psychiatric illness, or indeed for any group of patients or people other than those with intellectual disabilities or autism.
Definition of intellectual disability and autism
First of all, let me clarify what it means to have an intellectual disability or autism.
Intellectual disability is a lifelong condition that begins before adulthood, and results in impaired intelligence. People also have a significantly reduced ability to cope independently. It is a very broad spectrum. People will need varying degrees of support throughout their lives.
Autism spectrum disorder is a complex and usually lifelong developmental disorder. It is characterised by persistent difficulties with social communication and social interaction. Autistic people often find more difficult to build and maintain friendships. They also find it difficult to filter information, and can be over-sensitive to sounds or other sensory stimuli. Autistic people can find it very difficult to cope with changes of routine.
Although autism spectrum disorders are common among people with intellectual disabilities, not all people with autism have an intellectual disability. Asperger’s syndrome, for example, is a type of autism that is characterised by average or above-average intelligence.
Research evidence
Now let me tell you about my research. The aim of this presentation is not to promote a particular side of the assisted dying argument, but to contribute to the debate by discussing the implications, including the risks, for two particularly vulnerable patient groups. I am going to focus on three things:
the nature of the “intolerable suffering” that led to euthanasia requests from people with intellectual disabilities or autism in the Netherlands;
capacity assessments;
and the nature of healthcare inequalities internationally.
I will use the term “euthanasia”, as that is used in the Netherlands. It means a physician-administered death in response to a request from a patient to terminate their life. Whilst physician-assisted suicide is also possible, in over 96% of assisted dying cases, patients in the Netherlands opt for euthanasia rather than assisted suicide.
Case reports from the Netherlands
We analysed 38 case reports of people who had mild intellectual disabilities, autism, or both, and who died through physician-administered euthanasia between 2012 and 2020. These case reports are publicly available on the Dutch Euthanasia Review Committee website. As you will know, all cases of euthanasia in the Netherlands are reported to a Review Committee, who scrutinise them – typically over 6000 a year, of which an average 80 are published each year, with the specific aim to show how the committee applied and interpreted the legal due care criteria, and how they dealt with particular challenges.
The Dutch system of transparent reporting of euthanasia cases is unique in the world. In my view, this is essential in ensuring scrutiny and patient safety.
In our analysis, we focused on the question whether any particular difficulties arose when the euthanasia legal due care criteria were applied to patients who had an intellectual disability or autism spectrum disorder.
I can refer you to our published papers if you would like to know more details of our study, or indeed of the Dutch due care criteria and systems for scrutiny.
Intolerable suffering
My first examples illustrate my findings and considerations around the question of intolerable suffering without prospect of improvement, sometimes also translated as “hopeless” (this is part of the Dutch due care criteria).
In many cases, the suffering was described as not being able to keep up in society, feeling excluded from it, an inability to maintain relationships, depression, sadness and distress at not being the person they would like to be, and difficulty in coping with changing circumstances. People with autism had difficulty coping with what they experienced as an overload of stimuli, such as noise. For example, here are some quotes (the translation from the Dutch is mine). This is a man in his 70s with mild intellectual disability and autism who died through euthanasia in 2020:
Because of his autism, he found it increasingly difficult to cope with the changes around him. As he got older, he became less able to cope and his anxiety increased, eventually leading to intolerable suffering.
And a man in his 30s with Aspergers, who died in 2014:
The patient suffered from the fact that he had a great need for closeness with others whilst he couldn’t maintain long-lasting social contacts. This was because he misjudged interactions and was inclined to behaviour that crossed boundaries.
The difficulty here is that these patients’ suffering arose not from symptoms of an illness, but from the characteristics of autism or intellectual disability itself – as was the case for those who were highly dependent, had difficulties with social functioning, difficulties in coping with social circumstances, or a tendency not to cooperate with treatments. In a number of cases, physicians thought that further attempts at treatments or interventions were futile, as the patient wouldn’t cope with it, or would simply not cooperate.
Intellectual disability, with concomitant difficulties with social communication and relationships, could make it more difficult for patients to cope with the changes that come with ill health and ageing, or to weigh information, or to understand and accept possible alternatives.
In many of the case summaries, the term ‘suffering’ was used to describe the normal variations in behaviour and perceptions seen in people with autism which are an inherent part of the person. I could give you many more examples of this. Statements about the lack of prospect of improvement, such as “intractable symptoms”, “refractory to treatment” and “palliative treatment”, are meaningless in the context of lifelong disability.
So, one question I am raising is:
To what extent do the characteristics of certain groups of people make them eligible for assisted dying?
Or is the suffering described in these case reports in fact a result of society’s failure to accommodate and support the needs and characteristics of people with autism or intellectual disability?
Capacity assessments
My next examples are to illustrate the difficulties with assessments of the patient’s decisional capacity and competence. One was a woman with intellectual disabilities in her 30s who had a brain tumour in childhood, which had been in remission for 10 years. She was now suffering from unexplained physical symptoms, which one psychiatrist thought might be due to sadness that her life wasn’t what she had hoped. He found it difficult to assess her capacity, because of her coping style. This consisted of crying or indicating that she didn’t know, which made it very difficult to ask further about her euthanasia request.
There was disagreement between physicians about this patient’s capacity, which was not unusual in case reports where the patient had an intellectual disability. But she was granted euthanasia in 2020, because of the consistency of her request and the fact that she could describe alternatives to euthanasia. This is also not unusual.
A woman with intellectual disabilities in her 60s suffered from tinnitus. Her doctor had explained to her that most people learn to live with this, but, and I quote:
Because of her primitive thinking abilities, the patient was focused solely on eliminating the tinnitus completely. Once she realised ‘I will never get rid of it’, her suffering became intolerable and hopeless to her, and she was then only focused on euthanasia… She remained focused on her euthanasia wish, partly due to her low level of intelligence.
A persistent request does not necessarily imply capacity.
It might even be indicative of a lack of capacity, if the patient’s intellectual disability leads to difficulties in considering or weighing up alternatives. If stringent capacity assessment criteria were to be applied in this case, it may well be that the patient’s inability to appreciate the significance of the information in relation to her own situation, and to weigh up treatment options, would render her incapable to make a euthanasia decision, however persistent her request.
This takes me to the most commonly used and influential model for assessing whether a patient has the capacity to exercise autonomy in making healthcare choices: the MacArthur model, which consists of four abilities (also known as the “Appelbaum criteria”):
to understand the illness, the various treatment options and their potential benefits and risks;
to appreciate the significance of that information and how it applies to themselves in their personal situation;
to weigh up options usingreasoning and logic;
and to communicate a choice.
The difficulties many people with intellectual disabilities have in rationally manipulating information with regard to their situation, the consequences of their decision and the possible alternatives make them particularly vulnerable when the bar for capacity assessment is not set high. Of all four Appelbaum criteria, appreciation ability is undoubtedly the most difficult to understand and measure.
The problem is that impairment of decision-making capacity lies on a continuum, but the judgment of decision-making capacity is an all-or-nothing concept (either the patient has capacity to take a particular decision, or he doesn’t).
Where on the continuum the cut-off point for competence lies, is therefore a matter of judgement.
Many, including Appelbaum himself, have argued that the stringency of capacity tests should vary directly with the seriousness of the likely consequences of the patient’s decisions.
I would argue that euthanasia should only be open to those with a high degree of mental capacity to make such a request. For a life-or-death decision such as this, the bar for capacity should be set high. I am happy to discuss this further with you if you wish.
Health and social care inequalities
Finally, I want to point out that we have to be extremely conscious of the possibility of diagnostic overshadowing, where there is a negative bias impacting on a clinician’s judgement. There is strong evidence from around the world that people with intellectual disabilities or autism have been poorly treated and even died unnecessarily, due to poor decision-making by healthcare professionals. Numerous reports in recent years have suggested that the lives of people with an intellectual disability are valued less across society, and that their short life expectancy results from inappropriate value-laden decision-making by healthcare professionals.
When we look at the Dutch case reports, it was mostly accepted by doctors that suffering could consist of psychological pain, dependency, social isolation, loneliness and a lack of coping mechanisms that were a result of intellectual disability or autism. There were also several examples of rigid thinking, where the patient was fixated on the idea of euthanasia and unable or unwilling to consider alternatives. In the Netherlands, where most citizens are aware that they can ask for euthanasia if they feel their suffering is hopeless, it is inevitable that people with intellectual disabilities or autism can ask for it too; and as equal citizens, they have a right to do so. But the fact that the disability itself, rather than an acquired medical condition, can be accepted as a cause of suffering that justifies euthanasia is deeply worrying.
If the “intolerable suffering” does indeed result from living with the limitations of intellectual disability or autism spectrum disorder, then it is inevitable that it is hopeless. This, too, is evident from the case reports. In cases of persistent treatment refusal, or persisting problems despite having tried many different approaches and treatments, physicians tend to reach the conclusion that euthanasia is the only remaining option for the patient. In fact, many of the case reports were clear in their observation that autism is not a treatable condition, and therefore, the patient’s inability to cope with life was not treatable either, and therefore, euthanasia was a suitable option.
Bearing in mind the poor record of decision-making by healthcare professionals about people whose capacity is in question, who behave or communicate differently, or whose lives may seem to lack quality, I question whether such professionals are in fact the right people to make decisions about eligibility for assisted dying. Of course physicians can write clinical reports about the condition in question, but I would argue that the decision about eligibility should be one made in a legal setting, such as a court, after having heard evidence from the health professionals. There are many precedents for using the courts to make weighty decision, such as keeping a person in hospital or moving them to a residential setting against their will. This would provide prospective monitoring, i.e. before, not after, the death of the patient, and improved safeguarding.
I am in no doubt that the patients in the Dutch case reports did indeed suffer deeply and consistently. However, we know that people with disabilities experience severe inequalities in opportunities and in health and social care provision, which may well play a part in their situation being “hopeless”. Current society is not a level playing field, where everyone has a full range of life choices and can make autonomous choices about them. This makes it perhaps all too easy for people to request euthanasia, and to be granted such a death as a “way out” of painfully difficult situations and circumstances, rather than addressing underlying issues of inequality and a lack of adequate support for people with very complex needs.
I am not convinced that euthanasia was a suitable solution in most of the cases we reviewed.
I am going to come back to my initial question. You will have to be able to answer those two questions with clarity if you are going to make a sound decision.
Is changing the law safer and better for your citizens than not changing the law?
And what is your duty of care to your citizens who have disability?
At what point do you abandon your efforts to improve their quality of life and offer them an assisted death?
Thank you for listening, and I am happy to answer your questions.
Full details of the research cited in this presentation can be found here:
I never thought I’d see those words in the same sentence, during a pandemic no less:
LEARNING DISABILITY. GOOD WEEK.
But oh, the joy of those headlines.
Not just (as had been the case so far) those with Down Syndrome or those whose learning disability is severe or profound. Now, everyone who is on their GP’s Learning Disability Register will be fast-tracked for vaccination.
The relief that common sense has prevailed. Or (as the BBC1 newsreader announced it) people power has prevailed. It is an extraordinary turnaround, and worth pondering. How did this happen? What can we harness and build on? Because believe me, there are so many more turnarounds needed before people with learning disabilities are truly part of our society, treated equally, with equal chances of being healthy and happy.
What hasn’t prevailed, it seems, is a true understanding from the key scientists and policy makers of the nature of these inequalities, and indeed the nature of learning disability.
I was ecstatic on the day this news was announced. Messages flying around on social media and WhatsApp. My phone red-hot. My conversations with my colleagues, advisors and friends with learning disabilities were particularly wonderful.
Me: “Have you heard the news!” Amanda: “I have! My support worker told me! I can’t believe it!” Richard: “My news report last week on the BBC and Jo Whiley has done some good!” Vince: “It just goes to show that our voices can make a difference!”
(Here they are, speaking on the BBC news on 24th January)
So I nearly choked on my muesli when I read in the morning paper what Professor Anthony Harnden, deputy chair of the JCVI, had said: Despite adding everyone on learning disability registers to the priority list, people with mild learning disabilities should not approach their GP yet.
“We don’t want everybody with a relatively mild learning disability to come forward to be vaccinated now. That would cause problems because there are over 1.5 million of those individuals.”
Hang on a minute. Yes, there are well over a million people with learning disabilities in England, but that’s the best possible estimate. Less than a quarter (about 250,000) are registered with their GP as having a learning disability. This population is hidden, and that’s part of the problem. Those with mild learning disabilities are most likely to be part of this hidden group, yet they face significant barriers in accessing equal healthcare.
One and a half million people approaching their GP saying “I have a learning disability, please put me on the register, please give me the vaccine”? Wouldn’t that be brilliant. It would mean that they would be able to get a free annual health check, they would be asked what reasonable adjustments they need (more time for appointments? Easier information? Bring it on!). It is a dream scenario. It might be a good start in preventing future avoidable deaths.
The fact that this is seen as a nightmare scenario by the very people who advise on these matters, shows a worrying degree of mis-understanding about the root causes of inequalities in healthcare. Poorer health outcomes don’t just stem from underlying health conditions (although there are plenty of those to be had among people with learning disabilities). They also stem from people struggling to negotiate the healthcare system, unconscious bias among healthcare staff (we all have it, I’m no exception, it needs constant vigilance), and lack of reasonable adjustments.
So, all hail to People Power. The power of the media, too, in not just bringing this to the country’s attention, but keeping it in the headlines day after day. Jo Whiley and her sister Frances were, of course, the catalysts, and we cannot thank them enough. To talk to the media when you are torn apart by worry about your sister, fighting for her life in hospital, cannot be easy, however much you are a celebrity used to microphones.
But so many others were ready to back her up, as they have been campaigning for months. People with learning disabilities themselves, and their families and carers, were at the heart of this. So many have been shouting about their concerns and distress.
Mencap (who have now moved swiftly along to campaigning for people with learning disabilities to join the GP learning disability register. Share this if you can!). The PCPLD Network – we put out a campaign video in November and a vaccination webinar last month
Academics, supporting them with facts (like Professor Chris Hatton, for example, whose regular analysis of all the different and often confusing data I rely on).
But what was absolutely needed was the public to get behind it, and not shrug their shoulders: “Oh well, yes, very sad, but what can you do.”
I think what happened is that people began to see Frances as a PERSON.
Someone who matters, someone you really want and need to be part of your community and family, not in spite of who she is, but because of who she is. This message was also given by the mainstream news channels, who gave a voice to people with learning disabilities themselves as the main experts. (It was a joy to work with the BBC team on this!)
But unconscious bias remains. It is very hard to see the discrimination and disadvantage unless you are affected by it.
Being seen as “other”, less important, less worthy of saving (don’t even get me started on inappropriate DNAR orders), less worthy of vaccinating despite the evidence screaming of risk.
Perhaps it is telling even in the most innocent looking of news headlines, like this one: A huge relief for families…
You can’t argue with it. It is indeed a huge relief for families. But isn’t the relief greatest for people with learning disabilities themselves, who are now a step closer to seeing their families again, and to going back to the life they know? What this headline shows me is that many people can put themselves in Jo Whiley’s shoes, and that is a great step forward, but we are not there yet.
Like many of you, I have just watched the news and read the papers.
Finally, Public Health England has published their report on Covid-19 deaths of people with learning disabilities in England.
Here is the summary, and here is the full report. It is a review of available data on the deaths of people identified as having learning disabilities in England, from the start of the Covid-19 pandemic until early June 2020.
These numbers should make headline news. Here is Ciara Lawrence, who has a learning disability herself, speaking on Channel 4 News last night (and can I just say well done Ciara, but also well done Jon Snow for not only headlining this but including people with learning disabilities among the experts to comment on this report).
The rate of Covid-19 deaths among people with learning disabilities are estimated to be about 6.3 times higher than in the general population.
There are many estimates in the report, because there are so many ifs and buts, so many incomplete records and so much missing information. Most tricky of all is the fact that the majority of people with learning disabilities are hidden. Their learning disability is not noted in any records. The figure of “six times higher” is adjusted for those missing people. But even the most conservative estimates (looking at just the people with learning disabilities that we know about for sure) show that their death rate of Covid-19 is at least (AT LEAST) 2.3 times that of the general population. That’s the most conservative estimate, and shocking enough in itself.
If you are a young adult with learning disabilities (age 18-34), you are 30 times more likely to die of Covid-19.
Yes, you’ve read that right. THIRTY TIMES. It seems that the younger people with learning disabilities are, the greater the disparity with the general population. For higher age groups, the numbers are still very grim too. People with learning disabilities aged 35-44 are 19 times more likely to die of Covid-19. Those aged 45-64: 10 times more likely.
This pandemic is affecting the entire population of people with learning disabilities, not just the old.
I really don’t know what to say about all this.
Because haven’t we seen this coming? Haven’t we said it before, that people with learning disabilities are at huge risk, and we should pay attention?
The numbers on which this newly published report is based have been in the public domain for months. From families, learning disability organisations and campaigners to those with a real understanding of the numbers (thinking especially of Professor Chris Hatton here, who has kept us all looking at the numbers and thinking about the implications): Red flags have been waved since the early summer.
All I have now are questions. WHY and WHAT?
Why are these numbers so high? The report gives various possible reasons. Some of these are to do with physical health. The higher prevalence of health problems, such as diabetes and obesity. The fact that so many people with learning disabilities die of respiratory conditions, even before the pandemic.
Other possible reasons are social, emotional, cognitive and communication-related. The difficulty people may have in understanding and following lockdown restrictions and guidance on infection control. Or the challenges they have in communicating symptoms.
But the truth is, we don’t really know which of these factors have the greatest influence on death rates. That means that we don’t really know what’s the best way to address it.
What are we going to do about it? In a way the answer is obvious. Put resources into supporting and protecting this population. They should be right up there, on the VULNERABLE list. Of course care and protection needs to be individualised. Putting entire groups of people into isolation or give everyone the same shielding advice is not sensible. But what is sensible, is to ensure that all health and social care services recognise the dangers for this group of people. And most importantly: to ensure that they have the support and the resources to protect and support people with learning disabilities.
That means easy access to testing for all people with learning disabilities, staff and families. It means investing in giving people with learning disabilities the support they need to cope with lockdown measures. It means adjusting policies so that this can indeed be done. It may be that the very best person who can really help support someone with complex needs is a family carer currently prevented from visiting.
Among my many questions, there is a worry that this devastating report is going to be quietly forgotten. I have some niggles…
Why has it taken so long for this report to emerge? (The numbers were available in June. It is now November.)
And why isn’t this on the front page of all newspapers, and the headlines at all news channels?
I’m just imagining what would happen if the report had found this:
Students at universities in England, aged between 18 and 34, are 30 times more likely than non-students to die of Covid-19.
Can you see the headlines? The action? The investment in trying to understand this, reduce it, support students in whatever way was needed?
THAT is the kind of investment I want to see for the 1.5 million people with learning disabilities in the UK.
That’s how I started a blog post five months ago, when we were in full lockdown and the world was unfamiliar and scary. I don’t have to tell you about all the things that have been difficult, painful, stressful, worrying and just plain wrong.
But now, six months later, I come up from being submerged in a sea of strangeness, take a deep breath and look around at this new landscape. I still see things that are difficult, painful, stressful, worrying and just plain wrong. But I can also see something else.
Nothing like a pandemic to make us embrace new ways of connecting.
At long last! I’m writing a happy blog post about something positive!
A few days ago, the PCPLD Network hosted an online webinar. This is a great network of people who are championing the need and the right of people with learning disabilities to live the best and longest possible life, and then to have the best possible care and support at the end of it. I was the chair for a while (a position I’ve just handed over to Gemma Allen).
When the pandemic hit the world, we felt paralysed. Along with everyone else, we cancelled one thing after another.
We closed nominations for the Linda McEnhill Award scheme (we reckoned that the people who usually send us examples of outstanding practice – those working in palliative care services or learning disability services – had better things to do now than write nominations).
And we cancelled our conference, due to be held on 16th September in Cardiff. We were gutted. We had such excellent speakers lined up. Our conferences were our main networking events. If we couldn’t meet, how could we be a network?
PCPLD Network Conference in London (2018)
It seems obvious now that the thing to do is to host a webinar instead, but back in the spring, this felt new and scary. How would it work? Would anyone watch it? But as we had to hold and Annual General Meeting for our 300+ members, which could only really be done via video link, we thought we might as well try and add in a couple of online talks.
We would have expected some 150 people to attend our conference, so who knows, perhaps we could get that many people to attend online? Especially if we made it free, rather than the £100 we’d have to charge for a “real life” conference? (That’s what it would cost for us to break even on venue costs, speaker travel and hotel, delegate lunch etc).
Well, how about this.
Over 1400 people watched our webinar live, with many more catching up on it later.
If you’ve missed it, you can catch up too. Here it is.
The feedback has been so overwhelming. And all I can think now is: How amazing is that! Thousands of people all over the world who are connecting with these issues! Who are interested in finding out more, doing things better, sharing knowledge!
I am also thinking: Wow, this was hard work and lots of preparation, but now we know how to do it, we can do more!
I absolutely love it that this way, we can really communicate and talk to each other. I love it that we can include people in this who would never otherwise have been able to joins us, because conferences are:
too expensive
too far away
too time consuming
too intimidating (all these professionals!)
In our webinar, we could include the pre-recorded voices of people with learning disabilities and families, simply by holding a Zoom conversation with them. No-one refused. It’s so much less scary than standing up in front of an audience or speaking live online. (It also means that we could pare their talks down to the core messages, which was so much more impactful.)
Here’s an example of one such pre-recorded Zoom conversation, with my friend Richard. He had told me about a funeral he’d attended online, and how hard that was – so we simply talked about that once more on Zoom, and pressed RECORD. We used part of that clip in this trailer for the webinar:
We showed six such films during the webinar, each lasting just two minutes, and it was immensely impactful to hear the voices of these Speakers with Experience (experience of lockdown, and experience of having a learning disability). It also helped to keep the audience engaged.
I hope that you, too, are discovering the possibilities of this new online world. For what it’s worth, let me share with you what we’ve learned about putting on a successful webinar.
My top tips for webinars
1. Don’t do it alone. Get a team together.
Our team was just brilliant, sharing ideas for content and technical possibilities for months before the webinar. There was the PCPLD conference team of Gemma (our new chair), Louise Jenkins and Sharon Prowse, who brainstormed ideas for content. Anastasiya Stravolemova did all the technical stuff almost single-handedly, from editing videos to making sure the live event went without a hitch. For the live event, she enlisted the help of a colleague – so we had two “producers” behind the scenes, who sent speakers and videos and slides live at the right time. Louise monitored and published the comments that came into the Q&A box, whilst Gemma was busy live-tweeting the event. We had over 600 comments and Twitter went into overdrive, so both could have done with help! All I had to do on the day was sit in front of my computer and talk through my script, trusting the rest of the team to make it all work.
2. Choose your platform – and get to grips with it.
We thought about Zoom and Microsoft Team Meetings, but by now we were watching registrations climb well into triple figures, and most platforms have a limit on the number of attendees (although things are changing and improving all the time). We were incredibly lucky that Kingston University (where I work at the Faculty of Health, Social Care & Education) had just signed up to Microsoft Live Events, and not only agreed that we could use it, but helped us with the technical side (THANK YOU!!). They didn’t now what hit them. This was their biggest online event ever, so it was both interesting and hair raising to test this unfamiliar platform.
We practiced for hours. We tested everything, including the ability of external speakers to come on air. Just as well, as we discovered lots of things that could (and did) go wrong during those rehearsals. I won’t bore you with the details. We were so very happy when it paid off, and it all ran like clockwork on the day.
For recorded interviews with people who are not used to technology (and especially people with learning disabilities), I find Zoom is easiest.
3. Think carefully about your webinar content.
Have sympathy for your audience. It is much more difficult to keep your attention and focus when you’re sitting at a screen. It helps to have lots of variety of voices and things to look at. We were worried about asking Dr Kathryn Mannix to cut her planned one hour talk down to just 15 minutes, but were pleasantly surprised that this was effective. This particular webinar was quite complicated (only 1.5 hours to fit in 7 films, 3 speakers, Q&A and an online song!) and we won’t be able to go to that level of preparation more than once a year, but we’ll definitely think about incorporating several short sessions or speakers in future webinars.
We are planning more webinars!
By popular demand. There will be a monthly lunchtime webinar.
In fact I’ve spent today recording a couple of online conversations. Baroness Ilora Finlay‘s comments about Do Not Resuscitate caused some confusion among the listeners, and really needed more time and explanation. So I talked some more with her today, and also spoke with the mother of a severely disabled daughter about her experiences of being asked by doctors “Would you like us to resuscitate your daughter?”
I am incredibly excited by this brave new online world. How amazing that you can talk to a mother in the Netherlands, then show that conversation to an expert in Wales and get her to comment on it, all on a Sunday afternoon!
Oh, and this week I’m recording my first ever podcast, on “What words do you use when talking about death with people with learning disabilities?” That’s a novel venture for us, and I have no idea how it all works, but will give it a go.
So watch this space. And join us!
PS if you want to be kept up-to-date with all these future events, follow me on Twitter, or better still, become a member of the PCPLD Network. It’s free.











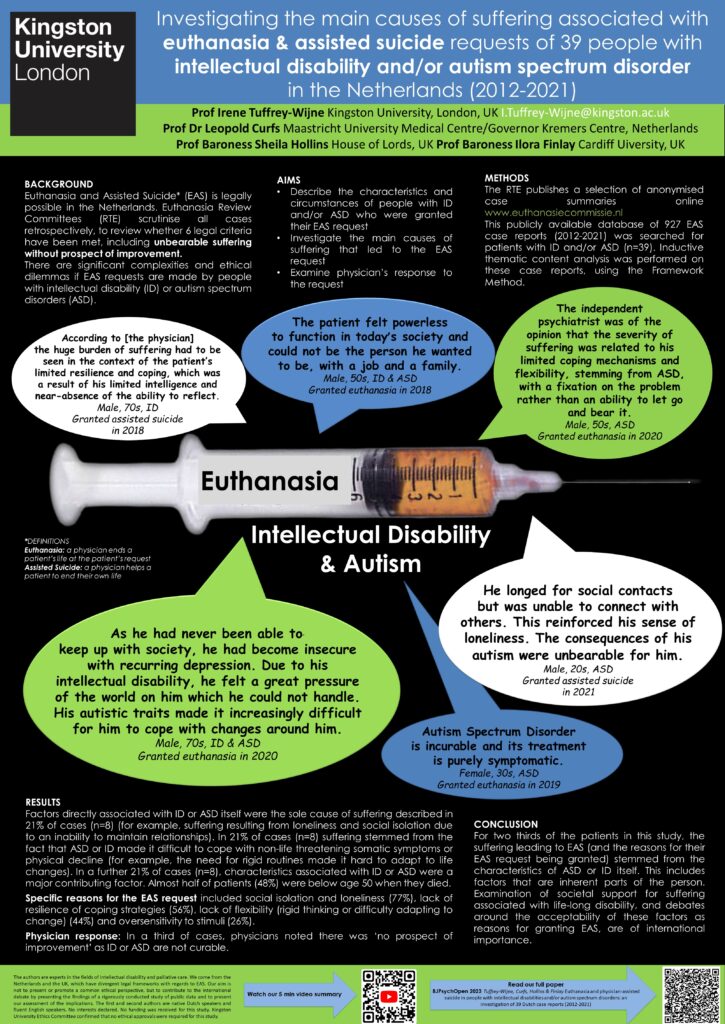



 We ended up with images like this:
We ended up with images like this: