I was at my Pilates class recently, trying to concentrate on my stomach muscles, when talk in this group of women of a certain age somehow turned to dementia.
What I fear most, one woman said whilst reaching for her toes, is losing all your dignity.
Yes! Yes, me too! said the others, before asking me, How about you? Aren’t you worried about that?
I thought about this, and I said no, I am not worried about losing my dignity.
Why not? Because I don’t believe I will lose it.
To me, dignity means being seen and valued as a human being. Being loved. Having the opportunity to do what I can do (whether that is looking after myself, making choices, maintaining relationships…) and help with what I cannot do (whether that is looking after myself, making choices, maintaining relationships…)
There was a time when I was unable to walk or feed myself. I had double incontinence and needed to be cleaned up several times a day. I was unable to form a coherent thought, let alone speak. Yet I didn’t feel undignified, and I’m 100% certain that nobody else would have said I lacked dignity.
That’s because at the time, I was a baby.
Yes, that’s me with my mum. I was 10 months old and really quite dignified.
Dignity is a relationship thing.
We give it to each other, by recognising each other’s worth and beauty, and the contribution we all make to the world simply by being in it. It has nothing to do with my ability wipe my own bottom, or to speak in full sentences, or to understand how the washing machine works. It has everything to do with other people understanding that I can’t wipe my own bottom, and doing it for me, along with my washing.
When I was a baby, my mother gave me dignity by loving me and caring for me.
When she was an old woman with dementia, I gave it back to her. When she was dying, she needed help with everything (yes, that included help with cleaning up after bowel movements and doing her washing). But she was never undignified, because she was always my mum.
With my mother in 2014, a few months before she died. Always dignified, despite her dementia.
Isn’t that life’s natural cycle? We need help when we start; we learn skills and use them; and we decline, losing those skills and needing help again. Some of us may need more help than others throughout our lives.
Loss of dignity is not related to disability, or dementia, or dying.
It seems to me that it is exactly the diversity of life that makes it so beautiful.
I know many people with profound disabilities who have never been, and never will be, able to wipe their own bottoms – yet they are profoundly dignified. (They might lose their dignity if there is no-one to wipe their bottom. That is a political point: there must be enough support for families, friends, carers and staff who are needed to help us all keep our dignity.)
Stephen Hawkins’ life was dignified, because people respected and valued him. They understood the things he couldn’t do for himself and helped him with those things.
In my line of work, people talk about “dying with dignity”. It crops up in the highly complicated debates on assisted dying.
I’d like to challenge you to think about this.
What does dying with dignity mean to you?
Does it mean being autonomous until the day you die, being able to do everything for yourself, being fully in control of every aspect of your life (and your death)?
Or do you think it is possible to live your final years in a dignified way, and die a dignified death, whilst needing help with things you can currently do for yourself?
If I live long enough, there is quite a good chance that I will get dementia. It runs in the family. My answer to the Pilates women is this:
I don’t fear losing my dignity.
What I fear is that I will be seen as a nameless Woman With Dementia, rather than Irene Who Happens To Have Dementia. It’s happened before – not the dementia bit, but the bit where you feel you are seen as a nameless patient, not a person. (In my case, a cancer patient. If you’re interested, you can read about that here.)
What I also fear is that I won’t be able to accept life’s cycle; that I’ll rail against it; that I’ll find it difficult to accept my limitations and difficult to accept help. It’s much easier for me to pretend to be Superwoman than to admit to myself that I’m not. (Quite a learning curve it was, my experience of being a Cancer Patient.) The way to help me (and you may interpret this as my Advance Care Plan) is to support me without fuss, and never to stop seeing me as Irene, however incapacitated or confused I might be.
A time may come when I might not recognise my son and daughters, but I hope I’ll still recognise their love. As long as they recognise me, and love me, I will have my dignity.
This blog post was first published by Marie Curie, see here.
Some of the challenges people with learning disabilities face when it comes to death and dying are hard to fix, but it seems to me that some solutions are outrageously obvious. Talking openly to people about death, and involving them in everything – including shared rituals of grieving – is one of them.
My friend Pete, who was terrified of death
Let me share the story of a good friend of mine. I’ll call him Pete. Pete had severe learning disabilities and he was terrified of death – perhaps because he watched his father die a painful death at home when he was a child. Or perhaps because when his mother died, Pete was on holiday. He wasn’t told that his mother had died until well after the funeral. Pete came back from holiday and found himself having to move, completely unexpectedly, to a residential home full of strangers.
Pete’s mother died decades ago. I keep hoping that Pete’s story is a history, but sometimes I still hear similar stories of exclusion.
A conspiracy of silence
When I was a hospice nurse in the 1990s, many of my patients had adult sons or daughters with learning disabilities, yet they rarely visited. My suggestion that they should was often met with alarm. Like Pete, many of the relatives with learning disabilities had not been told that their parent was ill, and certainly not that they were expected to die.
“She couldn’t possibly understand!” people would say. Or, “I don’t know how to tell her.” Or, “It will only upset him. What’s the point of doing that?”
Later, when I started doing research into all this, my co-researcher Gary Butler (who has learning disabilities himself) used to get particularly angry about this. “Of course he is going to be upset!” he’d say. “His father is going to die! Why aren’t we allowed to be upset?”
He’d go on to explain, “I know why. It’s because people don’t know how to cope when people with learning disabilities are upset.”
What should we be doing?
But talking openly about death and dying with people with learning disabilities is important. Most people cope best with difficult changes in their lives if they have some way of preparing for it, and if they are helped to understand what is happening. This includes telling people that someone close to them is likely to die, because otherwise, the death will be experienced as an unexpected, sudden death – which is much harder to cope with. Knowing that a loved one is going to die is sad, but sadness is not, in itself, a good enough reason to withhold such knowledge.
How to talk about death and dying with people with learning disabilities
Use simple words. Most people with learning disabilities I have spoken to about this, tell me that the best word to describe death is “DEAD”.
You can also use the person’s own vocabulary about death. Just make sure it’s their jargon, not yours.
Check with them what they think those words mean. If someone says “Mum’s gone to heaven”, ask what they think heaven is. It’s also worth checking their understanding of death. Do they think mum will ever come back from heaven?
Beware of euphemisms! “We lost dad” (why don’t we go looking for him then?). “He has gone to a better place” (Sounds nice. Why can’t I go there too?). One man I knew was excited about going to Devon for a holiday, as he thought it would be a chance to meet his friend who, he’d been told, had “gone to heaven”. A classic case of mishearing the words.
Some people don’t cope well with uncertainties (such as not knowing exactly when the person is going to die). This is particularly true for people with autism spectrum disorders. Think carefully about how to talk with them about what will happen in the future. It may help, for example, to go through a script (“We don’t know when Dad will die, but when he does, this and this and this will happen”). This can help in preparing someone to cope with what will be an upsetting time.
Talking is not the only way to explain what is happening. Visiting the ill person or, better still, involving the person with learning disabilities in caring for that person, can be extremely helpful. It can also give comfort after the death.
Remember that many people with learning disabilities will not initiate conversations about death, but that doesn’t mean they don’t want to talk about it. You can help by talking about the ill or deceased person in day-to-day conversation, helping people to share memories, etc.
Have a go. In the words of one of my advisors with learning disabilities:
“Tell the person the truth. Even if it’s bad news. Don’t be frightened!”
“I am a man with a learning difficulty. When I was about five or six, the headmaster at my school said that I couldn’t be taught.”
Now here is Richard a few days ago, the man who couldn’t be taught, having successfully completed our 8 week “How to do research” course for people with learning disabilities. At a university, no less. (Yes, he said, do put my picture on the internet.)
Ten students had come faithfully for two hours every week. We were blown away by their commitment, enthusiasm, questions and ideas. There were lots of punch-the-air-in-triumph moments over these past few months. For me, one of those was when a student said exactly this:
“I found that my hypothesis was wrong.”
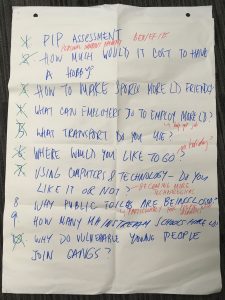
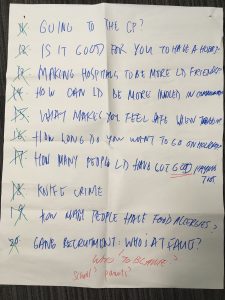
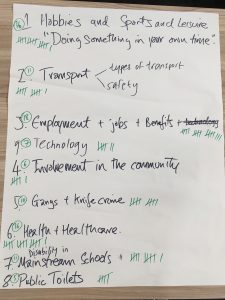
Now that’s a result. The students had come up with their very own research questions. Here’s the long list:
And, following a process of voting by the students, the winning topic was “Employment, jobs and benefits”.
Their research question boiled down to this:
“Why don’t more people with learning disabilities have good paid jobs?”
So, we split the students into three groups, each focusing on a different methodology. Three students worked on a questionnaire, to be handed out to their fellow students. None of these three students had paid jobs, so they worked out questions about this. To their surprise, they found that most of the respondents did have a paid job. Hence the student’s observation that his hypothesis (“People with learning disabilities don’t have paid jobs”) was wrong.
The students fill in the questionnaire
Another group of students worked on doing a one-to-one interview. They selected me as their participant. Their questions were brilliant (“What does this university do to support the employment of people with learning disabilities?”). Their interview skills were pretty good too, considering they’d only had a few hours to plan and practice.
Three students hold a face-to-face interview
(“Irene couldn’t really answer our question,” one student explained to her family afterwards. “Because they don’t employ people with learning disabilities at themoment.” Indeed we don’t. All my research funding applications over the past few years, that have included paid co-researchers, have failed.)
The third group of students worked on planning and facilitating a focus group. They, too, wanted the participants to be people with the power to decide whether to employ people with learning disabilities. Three of us (myself, a tutor and one of the students’ support workers) took part. Again, amazingly good questions, facilitating an excellent group discussion. (“What do you think makes a good employee? What stops you employing people with learning disabilities?”).
Three students facilitate a focus group
This course was an experiment.
I’ve wanted to do it for years. I’ve worked with people with learning disabilities as research advisors and co-researchers. It took me an entire decade to learn how they can truly contribute to and improve our studies, and what adjustments we had to make to ensure they can participate in a meaningful way. Research funders now require “user involvement” in research, but there is little guidance on how to make this happen in practice. Too often, the way we do research remains unchanged, with the Advisors With Learning Disabilities simply sitting in meetings that mostly go over their heads. As one of our contributors once said:
I don’t want to be there just because you want bums on seats.
I have gone a step further and worked with people with learning disabilities as co-facilitators of focus groups. We’ve also had co-researchers with learning disabilities help us interpret the data. But this takes time, and what we never had time for was to teach people properly. I, and most of my research colleagues, have had years of research training; but we somehow expect people with learning disabilities to join us and contribute, without any training at all.
How on earth are they supposed to know what research is?
What is the difference between a Research Question and any old question? What research methods to you choose, and why? What are the difficulties and the possibilities with each method? What makes a good interviewer? What do you need to think about when you run a focus group? What is the difference between open questions and closed questions, and when or why would you use them? How do you make sense of data?
I wondered whether we could really teach those skills. I wondered whether anyone was interested.
We applied for a small amount of grant funding from the NIHR Clinical Research Network, and received £3,000. This just about paid for Claire, my excellent research assistant, to prepare and deliver the course. I threw in my time for free, and two colleagues came to help out for a couple of the sessions. It enabled us to run the course free of charge for students. We reckoned we could accommodate ten students. We’d run it as a trial course.
Where to find these students? Would anyone be interested? I tweeted the information once and was inundated with interested people and organisations. In the end, we had 25 applications and selected 10 students at random. I had not foreseen the heartbreak for people who didn’t get in. One unsuccessful applicant telephoned me within minutes of receiving the email, telling me how hard it is to be always, always turned down for things.
I also hadn’t foreseen how much it would mean to the selected students, who (as we heard from Richard) have often been told that they were no good at school, to come to a university. My sister goes to university, one of them explained. And now I’m going too.
We treated them seriously, and they rose to it. Their confidence soared. Even the very-very-shy student stood up and spoke at the final session this week, presenting their work to family, friends and colleagues. Afterwards, their families and support workers told us that at home and in their jobs, too, their confidence had rocketed. For some students, who work for Mencap, it has already led to new research-related duties at work.
The students always arrived early, homework done, eager to start. And they were simply fabulous. Every week, I’ve been suprised by their insights and their ability to grasp quite complex concepts.
And we’ve had such fun!
They wept with laughter at the session on “Interview Skills” (and, more importantly, they remembered and incorporated those skills when they conducted their own interviews a few weeks later). Claire and I had role-played a very bad research interview, and got the students to hit a buzzer (making rude animal noises) every time they had a tip for me on how to improve my interview skills. Without us telling them anything about what makes a good interviewer, they came up with a pretty comprehensive list (all in the space of 15 minutes):
Eye contact!
Don’t talk about yourself all the time!
You’re putting words into her mouth!
Don’t look at your watch, or your phone!
This is not about you, it’s about her! If you make yourself look so important, it makes her feel bad!
If you’re asking a sensitive question, you have to explain why!
We filmed that session – you can watch it here.
What strikes me, watching it again, is that every single student contributes something useful at some point, from the most vocal to the most shy. For those students to tell me that I’m pretty rubbish and should do better, had the added benefit of giving them confidence that they can talk to a Learned Professor, and even correct her.
We sent them home that week with the instruction to hold a five minute interview with someone (on the same topic as our role play) and then come back to us with a list of Suggestions for Interviewers.
No need for us to write the Research Handbook. The students wrote it themselves.
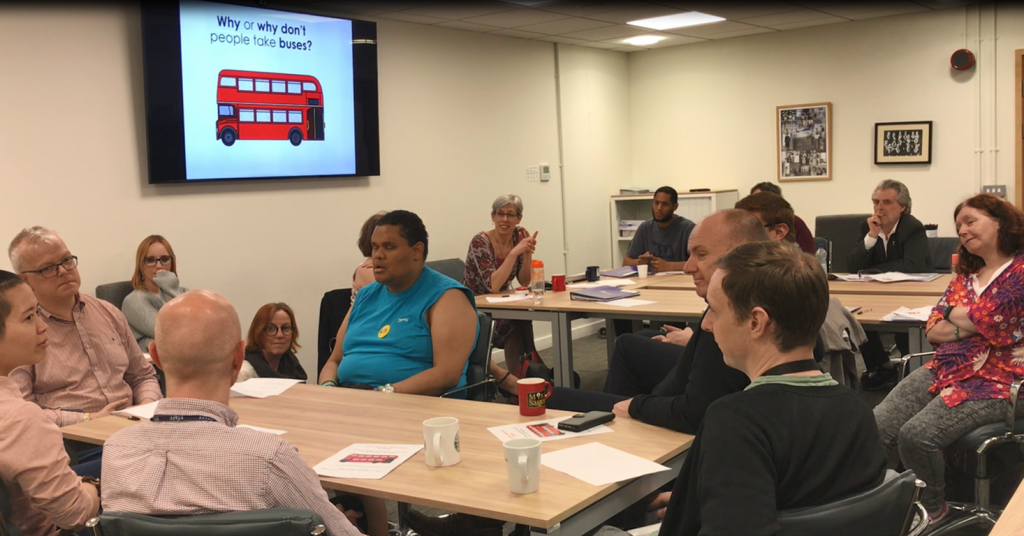
Similarly, the focus group week was impressive and fun. We’d grabbed a couple of colleagues in the office, to form a focus group for the students to practice on. (Our brief was that they’d been commissioned by a bus company to answer this research question: “Why do or don’t people take buses?”) The students soon discovered that facilitating a good discussion, where everyone contributes, is hard work. They noticed that one of the focus group participants talked too much about irrelevant stuff, whilst another said nothing. They took it in turns to try and do something about that.
(We’d been a bit sneaky, briefing our colleagues beforehand to give the students these challenges.)
Two of the students practice running a focus group, with the rest of us observing (and students taking over the “interviewer hot seat” if they had a suggestion for improvement)
The course finished this week. So what’s next?
I have already received enquiries from researchers who need people with learning disabilities to be co-researchers or advisors on projects they are planning. Would our students be able to do this? (Most students are interested in hearing about these kinds of opportunities, so I’ll pass it on to them).
In the autumn, we will write an academic article about the course. More or less all of the students want to come back and help us with that, so it will be a co-authored paper. We are also hoping to put together a short video about the course.
And we will make the course content available to others, so if you are interested in running a similar course, do get in touch. We’re happy for you to use our materials as long as you attribute it to Kingston & St George’s University. The more people with learning disabilities are trained in research, the better.
But really, what we should do is run this course again. And again.
There is clearly a need out there. All I need is someone to fund it. (We don’t want people with learning disabilities, who are usually on benefits or low incomes, to have to pay for such a course.)
I’d also love to expand. These 8 weeks have shown us that people with mild and moderate learning disabilitiesreally can be taught research skills, and that they are keen. We could only scratch the surface on this course. For those who discover that they really like research, it would be brilliant if we could run a longer, more in-depth course that would equip them to be great researchers. They could do it.
It has made me even more excited about possibilities for working with co-researchers in the future.
I have no research funding at the moment (as I said, I’ve failed spectacularly in recent years, with most of our grant applications turned down), so all I can do is dream… If only I could let funders understand that including co-researchers will make for the most brilliant research.
These students are not stupid. They really can learn, and they did. It’s just that they had never had an opportunity like this before, to learn complex skills in a serious but accessible way. They are rightly proud of their success, and we congratulate them.
I hope Richard’s headmaster, if he is still alive, reads my blog posts. I think he will find that his hypothesis was wrong.
Richard, if you are reading this: It wasn’t you who couldn’t be taught. It was the headmaster who couldn’t teach you.
It is the 1980s. A woman in her 50s screams as two strong men hold her down so that a nurse, who is 23 years old, can put a tube into the woman’s nose, all the way down into her stomach. She will be given an artificial feed.
The woman tries everything possible to resist. She doesn’t want to eat.
She hasn’t eaten for months. I don’t think anyone has tried to figure out why not. In any case, the woman never speaks.
This procedure happens twice a day. The place is a very large psychiatric hospital in the Netherlands, on a long-stay ward for the mentally handicapped. The burly men are a senior manager and a strong nursing assistant.
The young nurse is me.
I don’t remember the woman’s name. All I remember is that she had Down Syndrome.
Looking back three decades later, it is blindingly obvious that this was nothing short of ABUSE. If we heard of anything like this happening today, we would demand that the hospital was investigated and the nurse was dragged in front of a disciplinary panel, and possibly struck off the nursing register.
How on earth did I get to that point, the point of not only tolerating but taking part in abusive practice?
I was full of ideals. I had spent almost two years in the L’Arche Community in London, where people with mental handicaps (as it was then called) had become my friends. During my nursing training a few years earlier, I was told that I was paying too much attention to the young men and women in the institution where I was sent for my Mental Handicap Placement – it was a bad idea to become attached, bad for the “patients”, bad for me.
But now, in L’Arche, I had experienced our common humanity: the absolute importance of seeing each other as unique and important individuals.
Sharing a cuppa with Keith Lindsay (L’Arche London, 1985)
So, when I went back to the Netherlands and joined a nursing agency, I asked them to send me to work with the mentally handicapped (people weren’t yet called “people” in those days). The experience of not just spending time but sharing time with people with intellectual disabilities had been transformative. I wanted more of it. I wanted to share it with everyone.
I wanted to change the world, so that everyone would know everyone’s value.
It was a culture shock, to say the least, to find that people with intellectual disabilities lived in places that could not be called “home” in any way, shape or form. Where people were lined up naked in the corridor, waiting for their turn in the shower, never mind the builders and repair men walking past. (I was utterly horrified, but what do you do? How do you change it, as a young and unimportant agency nurse?)
It soon became clear that the ward staff, who prided themselves on being a wonderfully tight and supportive team, were supportive of each other, rather than of the people who lived on that ward. Those were not really people. The staff had built walls.
As the new person on shift, I wasn’t aware of those walls at first. I soon found myself on the wrong side (or, as I saw it even then, the right side).
There was the meal, shared around the table with some ten people including myself and another staff member. A particularly nice pudding was communally admired by sending it around the table, everyone taking a bite. Me too, when it was passed to me by the person I was sitting next to. My colleague was horrified, trying to save me from disaster by calling out “No! Don’t eat that, the patients have eaten from it!”
“Then why can’t I?” I said, and took my bite.
(What did she think I might catch? The Mental Handicap Virus?)
Then there was the trip to the swimming pool with the communal changing room. Together with another colleague, I helped three women to change into their costumes. Then I changed into my own. My colleague tried to stop me from the indignity of displaying my birth suit (“The staff changing rooms are over there!”) but I didn’t want to go there: “If they can change in here, then surely so can I?” People’s nakedness would only be undignified, I reckoned, if we made it so, by hiding our own nakedness in the staff changing room.
This was a temporary job. I couldn’t have lasted in that team. I would have been an outcast. It was hard, but my small acts of defiance, of trying to turn patients into people, kept me vaguely sane.
But then came the episode with the woman who was refusing to eat.
This was the real reason they needed an agency nurse. Putting in a nasogastric tube was a job for a trained nurse. It was the one thing I was required to do, which couldn’t be done by anyone else, because there were no other trained nurses on that ward. Articifial feeding was necessary, important, part of the plan for this woman. I wasn’t asked to do it; I was told to do it. By the most senior manager, no less, who came out of his office specifically to assist with the unpleasant task. Refusing to do this would mean I’d lose that job, and not only that, but my nursing agency would have been told that I was no good. End of career.
I didn’t think any of that through, though. I simply went with the flow. I did what was expected. I did as I was told. Clearly, everyone thought this was OK, so who was I to dispute it?
But coming home from those shifts, I cried and cried.
Day after day, I cried. It just didn’t seem right. I was devastated that the woman had to be treated in this way. There was no-one I could talk to about this. I probably couldn’t even explain why I thought it was all wrong. Weren’t we helping to keep this woman alive, by feeding her? What was the problem?
I was perhaps even more devastated that I couldn’t save the world. I thought I could live my ideals, living and working in a way that I knew was right, anywhere. But I found that I couldn’t. Faced with an overwhelmingly large institution, where staff were utterly institutionalised and patients were dehumanised, I had two options:
Let my ideals go, and become part of the system
Leave
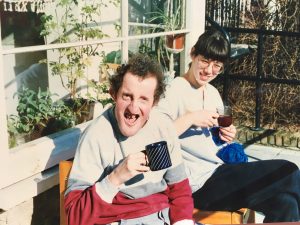
Readers, I left. Around that time, someone from L’Arche London telephoned me. The new home they had been renovating would soon be ready to welcome its first residents, and would I be interested in becoming House Leader? I didn’t need to think about it. I said yes on the spot. Some months later, I moved back to London and started visiting insitutions, just like the Dutch one I had escaped, to meet the people who would become our first residents. Including Carol Bell, who had grown up in such an institution. She was part of the (hopefully) last generation of men and women living their childhood and adulthood as patients rather than as people.
The reason I’m telling you all this now is that I have just forced myself to watch an old documentary about St Lawrence’s Hospital.
This is one of the asylums where society sent its “inadequates”. This is where Keith Lindsay grew up (the wonderful Keith – see photo above): I spotted him 44 seconds into the documentary. I knew it was a grim film to watch, but I didn’t realise quite how grim. Many of the people I’ve known have grown up here, or in similar places. They were profoundly deprived as children, utterly starved of attention and stimulation. It’s horrific. Carol and Michelle and Keith and so many other friends were, truly, survivors.
This film shows how horrid life was for the patients, but also for the staff, who needed to dissociate themselves completely in order to be able to cope. It’s a culture that turned nursing staff into zoo-keepers.
If you can bear it, do watch this film. It was filmed in 1981. That is very recent history. It is living memory. This is what our society thought we should do with people like Keith and Carol and Michelle.
We have come a long, long way, but we cannot be complacent.
Cultures and deep-seated attitudes are not easily changed, and still linger, as the alarmingly recent Winterbourne View scandal has shown. Cheer on the whistle-blowers, the campaigners, the quiet humanisers. I wish I’d been one of those whistle-blowers at the age of 23. I wish I could have done something better for that woman who was refusing to eat.
I couldn’t help her, but she certainly helped me. She was my turning point, the person who made me realise that I had to live my life differently. Sending me back to England, to be welcomed again by Michelle and Keith and other friends in L’Arche; and in turn, to welcome Carol. It is a tribute to the power of their human spirit that they not only survived the decades of deprivation, but thrived.
So thank you, woman-who-refused-to eat. I just wish I could remember your name.
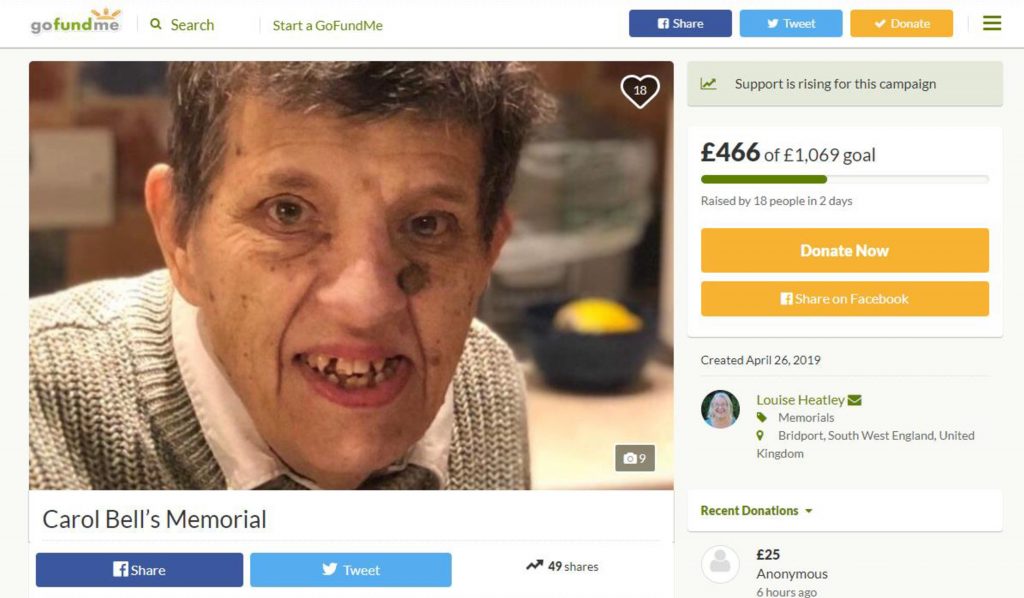
PS those of you who have followed Carol’s story, and seen her obituary in the Guardian, might like to know about the effort to raise funds for a crematorium plot and simple memorial at the local cemetery where her many friends can remember and mourn her. See here.
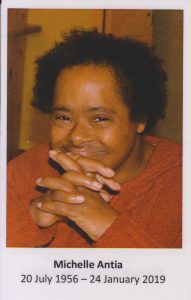
Here is the eulogy, given at Michelle’s funeral with such eloquence by our good friend Vivienne Frankish. Thank you, Vivienne, for letting me share it here: The story of Michelle’s life.
Vivienne gives the eulogy
Michelle, our belle…
Can it be that the force of nature that is Michelle Antia has been stilled, and our dear Michelle has completed her life, and that we are giving thanks and saying goodbye?
Michelle, possibly the most passionate woman I have ever known.
Michelle the loving, the hating, darting looks of fire –
Michelle the contemplative, the companionable, the survivor, the learner –
How to pay tribute to you, do you justice? There are so many stories – too many for now, but be assured, all of us who knew you will keep telling your stories for a very long time to come.
Let’s remember the very beginning.
Sadly, when you were born it was difficult for any mother or family to bring up a child with a learning disability. Resources were scarce, and mothers were advised to place their children in a specialist home and to forget them, to get on with their lives. So, as a child you lived in the Fountain Hospital, and as a teenager moved to Southside.
We know hardly anything of these years, just glimpses… Some favourite songs – You Are My Sunshine. Paper Roses. The way you write M for your name.
But signs, too, that people had not always been kind, and you had to find ways of surviving. Ways that challenged us.
There is one thing we do know about. An important friendship.
During all that long time you had a close friend, an inseparable friend – and her name is Janet.
In 1977, when the big hospitals were closing and “Janet” came to live in The Vine (the first house in the newly founded L’Arche community), because you were both inseparable, you came too. Lambeth Council wasn’t happy about it, but somehow our strong founding women, including Therese Vanier, made it happen.
And you began making the hundreds of friends who are remembering you today, here and across the world.
One of the founders of The Vine remembers that when Michelle first came, she loved the food but wasn’t keen on the idea of household tasks. She was outraged at the very thought of helping with the washing up, which she’d probably never had to do before…
Eventually, Michelle saw that her new lifestyle came with benefits. She began to settle in. There is an old Mencap film called A Home Of My Own, and some of it was filmed in The Vine. There we see a young Michelle, slowly, with great concentration and stillness, cutting up a cabbage for supper.
[Irene’s note: if anyone knows where to get a copy of that film, or indeed any old footage of the Fountain Hospital, Southside, or St Ebba’s Hospital where Carol lived, do let me know!]
I met Michelle 36 years ago in 1982. I was a workshop assistant. Michelle didn’t take much notice of me. We would sing along together as we worked. We’d weave little bags, and make tea and eat lunch. Janet and Michelle would play draughts after lunch with a Zen-like focus and I’d watch the checkers migrate off the board and down the table in a sequence of mysterious moves.
Again, in Michelle, that stillness…
Janet and Michelle by now had emerged from their close sisterhood into being their own people.
They each moved from The Vine to found a new L’Arche house. Michelle, together with “Fiona” and Nicki, founded The Sycamore. Others joined them soon after.
Michelle in “The Sycamore” household in 1985, a year after opening. Irene in front row (holding the cat); Nicki standing behind her, alongside “Fiona”. Keith (front row, far right) arranged all the flowers for the funeral; Nicki was there on the day Michelle died and helped carry the coffin; Marie (between Irene and Michelle) had travelled from afar; Fiona half-spoke-half-sang at the funeral service. John and another Keith (back row, far right and far left) have both died.
And this is where Michelle really blossomed and grew into her womanhood. It was a fusion of the right time, the right place, the right relationships.
Michelle became the local ambassador for L’Arche. The people next door held neighbourly gatherings – they were ‘something in the Foreign Office’. Michelle and Nicki were invited. Michelle knew exactly what was required of her as a guest. She was charming. She responded to being treated with dignity and respect by being dignified and engaging. A diplomat among the diplomats. Michelle was instrumental in helping the household establish its place in the street.
And it was while at The Sycamore that Michelle re-connected with her family.
Grandma was a regular visitor. Michelle was fiercely protective of her Grandma, and of Grandma’s handbag (glimpses again of how to keep precious things safe in the institution).
Through Grandma and Uncle, with a fair amount of detective work and inventive enquiry from assistants, Michelle made contact with her mum, who had left the UK a long time ago. When they took the plane and re-connected in Canada, Nicki remembers it was a natural, no-fuss occasion.
“Hello Mum.”
In time, Michelle met more of her family in Canada and the States. Michelle didn’t ask for much. Knowing that she had a place in her family, her family: that was what mattered.
Michelle was a parishioner here in St Matthews Church. She was confirmed here into her faith. Some of us noticed how Michelle carried a particular love, a devotion for Mary, mother of Jesus.
Michelle as Mary in the nativity story
Michelle had such a capacity for friendship.
She lived attraction and rejection at a profound level, and was vulnerable to falling in love. She longed for that someone special, just for her. She loved deeply. Sometimes she hated you at the same time.
Sometimes she just hated you.
(As we know, hate is not the opposite of love.)
Michelle with Carol
Some she loved passionately. Some, like her housemate Fiona, quietly, steadfastly. She had that ability to be alongside you, companionable and still, engrossed perhaps in her drawing and her writing.
I remember doing a collage with her on a retreat, and her chosen medium was digestive biscuits. We went into a kind of digestive biscuit meditation together. Michelle taught mindfulness classes.
And she could be a minx! The looks – the Who can keep this up the longest? – that often finished with dissolving into laughter.
And the craft workshop! She adored the Stonework. It was dusty work and we had special overalls, but Michelle was a dust magnet. She would be dusty from head to toe. The Sycamore assistants would complain, would make pleas on behalf of her hair care – but Michelle wore her dust with pride.
Michelle in the Stone workshop
She stood up for herself: Stop it. Don’t like it.
Loved doing new things: I’m learning! When she liked you: Cheeky Monkey. When she didn’t … Well, there was the kindly helper from a clown workshop who said, Michelle has chosen her clown name. It’s “Bucket”.
Michelle had her health difficulties.
She just got on with it. But the time came when ill health was getting in the way of her living the life she wanted, and so Michelle left her The Sycamore. It is a lovely house and indeed Michelle loved it, but she needed a home where she could move around easily without stairs and landings getting in the way.
So she moved to “Gowrie House” Care Home, and she created another community of new friends.
So many friends…
And we remember:
How Michelle was radiant when she was excited, pleased, happy.
How she loved her families, her birth family, her L’Arche family and her Gowrie House family.
How she created community around her. She insisted on it. When she was in hospital, all the nurses knew her and loved her.
At Gowrie House she would position herself at the hub of things, in the main room sitting next to her good friend Colette, or in the office with the staff, or upstairs with Ann, her favourite staff member, working alongside her.
She was poorly such a lot in these last few years. Each time we thought, This time she won’t recover, and each time she did. She surprised us again and again.
Irene with Michelle in 2018
In the end she surprised us, by dying so quickly, so peacefully, finally letting go.
Her life complete.
Michelle taught us how to see her – and she continued in her teaching even after she died. Helping the staff at Gowrie House, who loved her and cared for her so well, to find a way to say their thanks and goodbyes. And for her friend, Colette, to bless her journey with a prayer.
Michelle: a tempestuous lady, with a quality of stillness, of presence and connectedness.
Michelle, who always stayed true to herself and was not going to be bent out of shape for anyone.
Here I am. See me as I am. I am complex, and I am so worth getting to know.
After she died, I and others sensed her qualities of stillness and connectedness there in the room.
Michelle, we thank you. We love you.
You will be in our thoughts whenever we sing Michelle Ma Belle, our beautiful, passionate, compassionate, complex companion and friend.
For these past few weeks, I’ve been floating in a fog of funerals and farewells from which I’m not quite ready to emerge. Trying to have some rest and restoration this weekend, so I’ll be able to focus on work again on Monday (there’s a research funding bid to write, for starters), I find myself thrown back into the mist every time I try to look into the sun. There are still more stories to tell.
Completing this series of blogs, there is Michelle‘s farewell, and then Michelle’s life to tell you about (I’ll share her eulogy tomorrow).
There may well be postscripts, too. I’ve learned more about life, death and intellectual disability in these past few weeks than I’ve learned in the past few years of research.
Michelle’s funeral was an exuberant, sad, uplifting, publicly intimate affair.
It had something of the home-spun about it. We did it ourselves, said Michelle’s friend Louise, with whom I carried Michelle’s coffin into church. It was a different church from the one where Carol’s funeral was held five days earlier, but here, too, there was standing room only. We sang our hearts out.
Michelle’s friends were many and spanned a lifetime.
Her oldest friend Janet (that’s not her real name) had shared Michelle’s life since they were both little girls. They grew up together in hospital, like sisters. So inseparable, in fact, that it was blindingly obvious to everyone (except perhaps the local council who had to fund it) that when Janet came to live in L’Arche London, Michelle had to come too.
Janet herself is now in the winter of her life, the days closing. It is difficult to know how she understood Michelle’s death (can any of us understand it?), but it was deeply moving to see her stand in front of her soulmate’s coffin, sing a song, say an Amen, then walk away with such dignity.
Janet at Michelle’s funeral
Michelle’s good friend from her L’Arche years, holding up a framed photo when we all gathered for Michelle’s “wake”, the evening before the funeral, telling stories, remembering. Remembering the friendship.
She was the best friend I’ll ever have. I’ll miss her.
Michelle’s friend shows us her treasured photograph
We weren’t sure whether anyone from Michelle’s family could make it, so we were astonished to see Michelle’s mother turn up unexpectedly early for the wake. Hers had not been an easy story. Like Carol’s family, she had to cope with leaving her small daughter in an institution – and then disappeared from the scene completely. In her L’Arche years, Michelle found “mummy” again, now living thousands of miles away. There were several jet-setting holidays to Canada and the States. Today, mummy is in her eighties and frail. To have made it across the ocean is nothing short of miraculous.
One of the friends missing from that evening of remembering was Colette, who had become so close to Michelle during the last few years in the Care Home.
(Colette’s story clearly struck a chord with you all – the blog post describing the conversation I had with her, the day Michelle died, has been seen almost 25,000 times on Twitter.)
I’d telephoned the Care Home several times, urging them to ensure that staff and residents came to this gathering, if not the funeral.
Even if they don’t want to stay, I explained. That will be fine. People will be wandering in and out, making noises, crying or laughing, it doesn’t matter. Please let Michelle’s friends come. Please let Colette come.
But Colette’s family was there. Her sisters, deeply moved by this messy, heartfelt, tender time of sharing memories and belting out Michelle’s favourite songs (Edelweiss! Michelle Ma Belle! You Are My Sunshine!), agreed. Colette should have been there.
They brought Colette to the funeral to following morning.
The funeral was both well-planned and spontaneous, with space for Colette to come forward with her sister. She gave an impromptu speech, with words that were strikingly similar to those of the friend the night before.
She was the best friend I’ll ever have, Colette said to everyone in the church, having wheeled herself right in front of Michelle’s coffin and facing us all. We do colouring together. She was my best friend. Jesus, look after her for me.
Amen, we said to that.
And then Colette’s sister, after sharing a few of her own memories of Michelle in the Care Home, turned to Michelle’s mother (whom she had met the evening before) and addressed her directly.
Now that I’ve met you, she said, I can see where Michelle gets her beauty from. Thank you for Michelle.
Was this the most moving moment of all these deeply moving days? I think it was.
I know how difficult it is, Colette’s sister said, to make the decision to send your child with disabilities to live somewhere else. I’ve seen how hard it was for my own mother to make that decision. The guilt. But look at all these people here. Look how amazing Michelle’s life has been, and how many people love her. That wouldn’t have happened otherwise. So please don’t feel guilty. Thank you for giving Michelle to us.
Michelle’s mother reached for her hanky. So did I. So did many of us.
These foggy days of funerals and farewells can (dare I say it) be a time of healing.
If we look death and loss in the face, if we can share our distress, our guilt, our if-only’s, but also our joy at having known and loved this person, if we dare to sit for a while in the new hole in our lives, then that really helps us. It’s helped me. I’ve explored the hole, so now I can recognise it. I’ll still fall into it, but I’ll know how to get out.
(Finding others who know the shape of that hole too. That’s how I get out.)
It has helped me to understand the lives of my two friends, Carol and Michelle, and to see how much sense those lives have made. How they are complete. Seeing that completeness, and indeed seeing how the very heartbreak of their stories are an essential part of the completeness, has also helped me. It is a comfort.
So I’m on a mission. In our recent Talking About Dying Survey, we asked support staff across the UK whether bereaved people with learning disabilities were involved in funerals.
We found that most people with learning disabilities now attend the funeral of someone close to them, but very few participate in them.
Even if it is the funeral of a parent, say. Very few people were involved in planning it, choosing songs or flowers, saying a few words, helping to carry the coffin. Few people with learning disabilities, it seems, are helped to take their place as principal and active mourners.
If you are not convinced that it is possible to include a very diverse group of friends and family in the rituals of farewell, do watch this short video of Michelle’s wake and funeral. Gloriously, it starts with a very short clip of Michelle herself, singing along to Edelweiss. We have been singing it a lot during these past few weeks…
I had the enormous privilege of giving the eulogy at Carol’s funeral this week. It was followed by a personal reflection, given by Chris Sadler.
Chris and I had the difficult task of visiting several people living in large institutions in 1989, and deciding whether they would be the right people to move into Gothic Lodge, our almost-ready new L’Arche Community home for six people with severe and profound learning disabilities.
At the time I thought we chose Carol. Now, I think she chose us.
For those of you who have been asking: Here are our words in full.
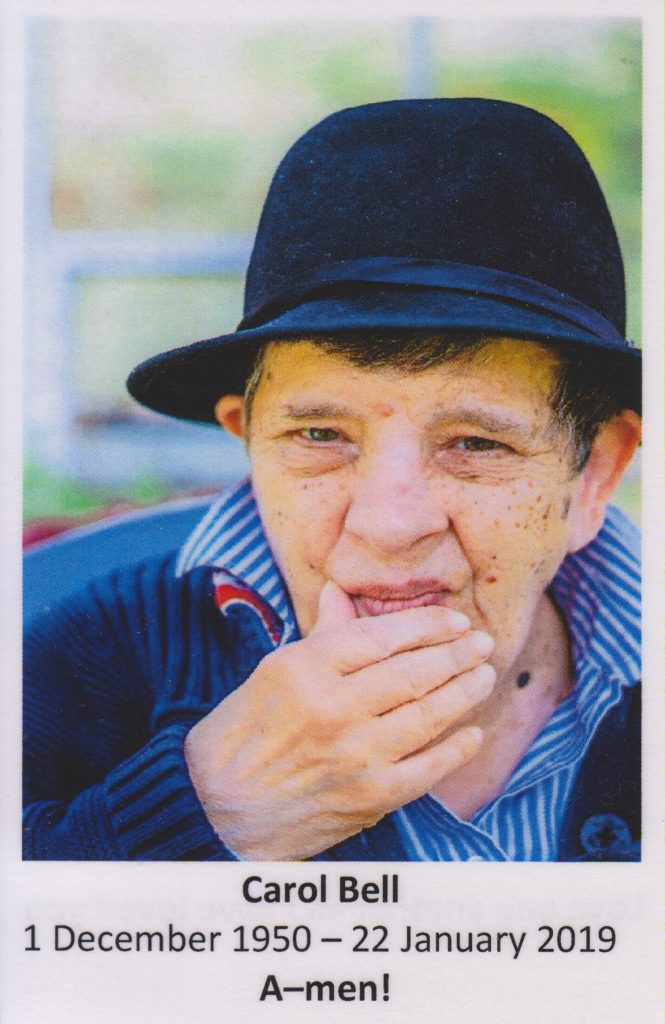
Eulogy for Carol Bell, given by Irene Tuffrey-Wijne
Carol Ann Bell.
Look at all these people here, gathered to mourn your life, and celebrate your life, and laugh and cry about your life, because you touched theirs. Look at the many people all over the world, who wanted to be here, but couldn’t make it. Look at all these hats!
Carol’s birthday, hugely anticipated and celebrated every year, was on 1st December 1950.
She was the second of seven children.
And she was loved. Carol’s mother loved babies, and she loved Carol.
But to be a child with disabilities in the 1950s was hard, and to be the family of a child with disabilities was also unbearably hard.
In those days, babies and young children with disabilities were put away in large institutions. Families were told that it was best for the child to be “with her own kind”, and it was best if their families forgot about them and never visited again, because family visits – and especially family departures – were just too upsetting.
Carol’s mum didn’t want to give Carol up.
But in the end she had to, because there was no support, and she was struggling to cope, carrying this toddler up the stairs, with an older child and another baby on the way. Carol went into a large institution at the age of two. And she lived there until she was 39.
We know very little about these years. Records were lost. Much of Carol’s life was lost.
But we do know that her mother defied the establishment’s advice. She visited Carol for years, taking the long, long walk to the hospital, sometimes taking one of her other children along.
In a way, Carol’s mum never gave Carol up.
We know now that those hospitals were dreadful places to live. Years later, Carol’s mum and one of her siblings who remembers this, told me that they were also dreadful places to visit. That they managed it at all is amazing, because most families didn’t. But in the end, it simply was too hard and too upsetting, not just for Carol but also for her mum. She stopped visiting when Carol was about 20 years old.
But she held Carol in her heart, always.
Chris Sadler and I first met Carol when she lived in St Ebba’s hospital in Epsom.
At some point, St Ebba’s had over 600 beds for “mentally subnormal patients”. The hospital was finally closing, with residents moving into small homes in the community.
We walked into the large lino-floored room with about a dozen women in it, and she watched us like a hawk. Who would we go to? She knew that if strangers came onto that ward, they usually came to meet a fellow resident, and that resident would soon move out. She was completely delighted that we came to see HER. It was her lucky day.
Of course we all know, now, that it was really OUR lucky day. We were so lucky to have found Carol.
That day, Carol showed us around the hospital grounds. The first thing she did was to drag us to another ward, to introduce us to “My Friend”. This was a man in a wheelchair, who was unable to talk. It was clear, even then, that Carol had a gift for friendship, as well as a gift for community. She wanted us newcomers to know her friends. She must have had many friends in that hospital.
Carol moved into Gothic Lodge in 1989. It was a drastic new beginning.
Carol’s first day in Gothic Lodge, 1989 (with Chris)
Sadly, her old friendships were lost. We were unable to keep track of her friends. All she had with her was a dustbin liner with a set of brand new clothes, and memories she was unable to tell us about. 39 years of her life were erased and lost.
We think her memories were, and remained, vivid. We had glimpses.
Carol was a great observer, and a compassionate observer. We think she must have honed those skills in the hospital, where she saw many people in need, and indeed people dying. In later years, she would sometimes show us this by acting it out.
Philip, Chris and myself had just moved into Gothic Lodge. So had Sunta, Betty, and several others. Laurence and Terry arrived over the next few weeks.
The Gothic Lodge household in 1990 (Carol in front, 3rd right)
We told Carol that Gothic Lodge was her home. And so it turned out to be. Over the years, she became the centre of gravity in her home. She became the home maker, the welcomer.
And to Carol’s great joy, and that of her mother, contact with her mum was re-established after a 20 year gap.
Carol and her mother in 1990, reunited after 20 years
Many of us feel guilty or regretful about having had Carol in our lives, but not being in contact much. But Carol never held a grudge. She didn’t look at the years she hadn’t seen you. She was simply utterly delighted to see you now, as if you’d never been away.
To her equally great joy, years later she also found her siblings again, when they all met up at their mother’s funeral. Carol loved going to stay with Jim and Marie in Kent, with Dave in Blackpool (who sadly died last year). She loved her nieces, and their children. Young Robson who loved getting her shoes for her, and helping her put on her coat, and holding her hand when they went out.
It is amazing that despite the years of forced separation, Carol was, in her family’s words, “a true Bell”. I’m told that once the Bells make their minds up, that is it!
Carol shared her mother’s love of babies. She shared the Bell sense of humour, their love of animals, and of horror movies, and of Kung Fu Fighting.
It was a joy to welcome Carol, but it wasn’t always easy in the early years in Gothic Lodge.
It took a long, long time for Carol to believe that this was her true home, with friends who loved her. She would spend night after night curled up asleep on the floor outside Chris’ bedroom, perhaps making sure that we stayed in her life. Whenever Chris went away for a few days, Carol would go into Chris’ bedroom, just to check that all her things were still there and Chris hadn’t disappeared.
“You come back!”is an instruction many of us have ringing in our ears.
In the 29 years Carol lived in Gothic Lodge, she welcomed hundreds of new people into her home and her life.
Some for a few months, some for a few years. Many became lifelong friends. The visitors she welcomed cannot be counted, but I’m pretty sure they all remember her.
How are you? she’d ask. What’s your name?
She wanted to know not just how you were, but who you were, and how you fitted into the fabric of life.
How’s your mum? How’s your dog? she would remember to ask.
Carol noticed people being unsure, or alone, or new to the group.
She would go to them and make sure they became part of things. And when people were unwell or sad, she knew it before anyone else, and she reached out to them, and worried about them.
I’m grateful to Pauline for letting me tell her story, because it illustrates so powerfully this beautiful gift of shared humanity that Carol had.
Pauline lived in Gothic Lodge in the early years, and remembers the time when she had a serious breakdown. Pauline was upstairs in her bedroom, lying on a mattress on the floor, very unwell. Nobody knew what to do. People came into the room with offers of talk, of food. None of it was any good.
Carol came in, sat on the end of the bed, and turned the telly on. And sat. Sometimes she’d look around at Pauline and nod at her. That’s all.
Carol was the one person who could sit with you. She saw your need.
And it wasn’t limited to people… There’s the story of the chicken being prepared for Sunday lunch. Carol looked at it and said, “Poor chicken! Not well!”
Carol’s joys in life were simple, easy to achieve, easy to share.
Watching and re-watching her favourite film for the 100th time. Any suggestion of a different film this time, would be very firmly declined.
Watching Casualty with Terry on a Saturday night. Regular trips to the local café. Cappucino. Sausages. Chips. Ice cream. Maltesers. Her love of the seaside and the cinema. Of music, singing songs. Of dogs and horses. Of babies and children. Of soft toys, the bigger the better. Her love of hats.
Her love of pilgrimage, belting out songs at the top of her voice whilst walking down the country lanes to Canterbury.
The care she took making everyone tea. Taking orders, boiling the kettle, laying the tray. The mugs would be over-filled, some would have 2 teabags in, the water off the boil, but it was done with such time and care and attention, making sure everyone had a suitable mug.
Her love of parties. Especially birthday parties. Especially her own on the 1st of December. By me, was all her friends needed to hear to know they were invited, quite possibly as early as August.
How she could say No more! with such cheer and good humour, yet so firmly.
And Carol was funny, often hilariously so.
It wasn’t just in L’Arche that Carol built community. She was also a faithful member of this church, the community of All Saints.
Here, even the parishioners who didn’t know Carol, know Carol, because of the way she made herself completely and comfortably at home in this church. Installing herself in the front row. Striding up and down the aisle, shaking everybody’s hand. Bringing up the offertory and kissing the priest at the end of it.
And of course: her very loud A-men!
Carol lived a life of endurance and determination. Whatever the difficulties and the losses, she never gave up.
And Carol’s life, in the end, had come full circle. She had found her family, which is perhaps all she ever yearned for. She finally understood her place in the world, and she was at peace with her place. What a joy when her family managed to get to her 68th birthday party, just two months ago.
In the lost years of her life, Carol honed her skills of compassion and bloody-mindedness.
In the community years of her life, Carol honed the skills of friendship and of welcome. She was a community builder. Perhaps it was Carol’s mission to befriend people, including generations of young people. To teach them about acceptance and about loyal friendship, and then send them out into the world, changed by it.
Carol had a strong need to belong, and in searching to belong, she drew us in and helped us to belong too.
We will miss her more than we can say.
Carol died with a song and a prayer, surrounded by a community of friends.
That is a comfort to us. For many people here, it is also a comfort to think of Carol in heaven. Her delight in seeing so many friends there, and of course her mum and her brother David. It is a comfort to think that just 38 hours after her own arrival, she was first in line to welcome Michelle.
And it is a comfort to imagine how, when our time comes, Carol will have forced herself to the front of the crowd to reach out and welcome us. She will name us, and she will say, THERE you are!
She will probably drag us right into the centre of Heaven, and introduce us to everyone, just to make absolutely sure (once more) that we, too, belong, and like her, we, too, have found home.
(Irene Tuffrey-Wijne)
Personal reflection on Carol Bell’s life and friendship, given by Chris Sadler
I guess many of us here can say Carol was my friend.
Some of us who knew her well can say, and she was my teacher.
This is a personal witness to her friendship and teaching.
After Irene and I visited Carol in St Ebba’s Hospital, there were more delays to the renovations of Gothic Lodge. One day a call from St Ebba’s Hospital. Carol would not stop talking about going to a new home, hundreds of times every day, for months. When could she come, they pleaded?
Finally she arrived. I think we imagined welcome would be easy. After all, she wanted to come.
We did not remember what a shock it can be to arrive in L’Arche. So many new people, so many strange ways. She was not in control. I think it awakened her vulnerability, her deepest needs.
In her confusion, Carol glued herself to me, and stuck for years. As an extreme introvert it was not really my idea of friendship. I cringe remembering the countless times I said, Stop it. Leave me alone. I’ve told you.
I did not understand much about attachment theory then. It took time to realise I hated the clamour of her incessant needs partly because, unlike her, I had no idea what I myself really needed, let alone how to ask. Then a wise person said to me, When someone keeps repeating the same thing over and over again, it is not because they have not heard your reply. It might be because you have not heard what they are really asking or needing.
What if Carol was asking:
Do you really care? Enough to love me? Enough to let me be a faithful friend to you? To be with you when the chips are down?
Carol and Chris in the early days
Carol brought some order into her strange new life, by importing old routines from St Ebba’s.
At night she folded her clothes impeccably ready for the next day. In the morning she made her bed before breakfast. We glimpsed other routines of institutional life. If she considered someone had misbehaved, she would mimic, Ignore him. No party for you.
In another life she could have been a very bossy teacher, a control freak, Lady of the Manor, or a Kung Fu fighter. But other qualities were emerging.
She was curious. She observed deeply. She read our faces, saw our hurts, felt our feelings.
She gave us our own unique names. Sometimes she tried one of us on like a costume: it was her gift of empathy. At other times when she mimicked someone with amazing accuracy, it was pure fun and she knew it.
But when she held a baby in her arms she had a timeless gaze.
Was there anyone who lived in Gothic Lodge or worked with her, that Carol forgot? I doubt it. If a connection was made it was for life, and it included all of us, all our failures of attention or kindness, even our leaving.
She forgave all.
Carol was not timid, always ready for an adventure: her first plane, her first pilgrimage, new beds, and new people were always exciting. True, years later, being unsteady on her feet was scary. Would she be upset or feel diminished at using a wheelchair? Just the opposite: she was liberated. She could give all her attention to life around her. She was empowered: she could wave, nod, give directions, be queen of ice cream. She could again visit her many friends in their homes, in pubs, riverside cafes, at church.
Still it is important to say Carol was for much of her life acquainted with grief, with the suffering and dying and leaving of her friends. And with the suffering of her own body, the recurring cycles of Not well…better now.
Where did she learn so much resilience and courage?
Who taught her that mysterious and holy thing that has been around so strongly as we remember her and Michelle?
The nearest name I can find for it is grateful-sadness or perhaps joyful grief.
Where did she learn such total forgiveness?
Where did she learn such faithfulness (and still keep her delicious wicked humour)?
Where did she learn such tenderness, such compassionate presence?
Who taught her to be as sound and clear as a Bell?
Certainly she learned if with her mother, continued and shared with her beloved family.
She learned these things from her own amazing spirit, from the repertoire of songs that lit up her life, her musical soul.
She learned it from her lifetime practice of welcome.
She learned it, I believe from her baptism. It was visible in her radiant face and as she said Thank you Bobert to the vicar, and hugged the three friends who held hands around the font the evening before her Confirmation here in All Saints.
She learned it from, and taught it back to us, in L’Arche, and here in All Saints Church.
I would like to honour one other person from the hidden years of her institutional life. One of many whose names we do not know, but Carol never forgot.
I noticed in the early years at Gothic Lodge she did not really answer to “Carol”. Sometimes when she felt she had done well, she’d mutter to herself, Good girl, Bell. I remembered something form that visit to St Ebba’s hospital. One of the less senior staff, who had been around awhile, mentioned that a woman who worked there for many years, dearly cared for Carol. Perhaps she was the one who called her “Bell” kindly.
Carol apparently was distraught when this woman left (or died).
But, and this is important, not so distraught and devastated that she could not trust again in friendship.
Some of us feel distraught today, but we have a teacher, a teacher of welcome, of “joyful-grief” of friendship stronger than death.
Carol Bell, as you said so often to others, I say now to you:
Thank you, thank you for coming.
(Chris Sadler)
For a short film with extracts of the funeral service, see here:
There was standing room only at Carol’s funeral yesterday. Well over 200 people had come from near and far (some from very far) to celebrate her life and mourn her death. The funeral service lasted almost two hours and was not a minute too long – so much to say, so much to sing, so much to pray.
“I just can’t explain to others why I’m so upset about Carol,” one young man said last night at Carol’s home, where – after the funeral and the cremation and the sandwiches and the tea – some of us had gathered for sausages & mash & wine. He, like most of us round the table, had once lived in this house, together with Carol.
“They ask, Who is Carol? and all I can tell them is, Woman in her sixties, severe learning disabilities, lives in a care home. She died.” And my colleagues and friends look completely blank, wondering why on earth that matters. But it matters! It matters so much!”
There were vigorous nods of recognition. We have all heard the unspoken assumptions from people who have never met Carol or Michelle or indeed anyone else with learning disabilities.The assumption that really, deep down, isn’t the death of an elderly woman with such severe disabilities a blessed relief?
But look. The people who turned up for Carol’s funeral were not just members of the London L’Arche community, where she lived. They were also members of her family (lost during the first half of her life, when she lived in an institution, but found again in the latter half). They were parishioners, surprisingly many of whom had turned out on this Thursday morning. They were neighbours, people who simply knew Carol because she lived in their street.
They felt blessed, perhaps – but they certainly didn’t feel relieved.
Two hours of tears and laughter, and then more tears as we listened to Nunc Dimittis and sang as Carol’s friends and family finally carried her out of the church.
Oh, she matters. I had the huge privilege of giving the eulogy, telling the story of Carol’s life, which I will share with you in my next blog post. Because it is important that we recognise the important place people like Carol have in this world.
It seems to me that I appreciate only now just how big that place was. How huge the Carol-shaped hole that I am now staring at. I’ve been thinking about her life, I’ve been listening to so many Carol stories, and only now do I see, clear as anything, just how and where Carol fits into the bigger scheme of things.
But not only that: I see how Carol and Michelle fit into my life, and how they have shaped the person I am today.
With death and grief comes new understanding, a better understanding of who we are, and where we ourselves fit into the world.
Carol’s need for relationships and community was so strong that it was impossible not to be touched by her. I know there are many people in the world, people with severe learning disabilities like Carol, who touch those around them. Not only their families and carers, but also (if given the chance) people in their wider community. They are able to draw us into a different way of relating, sharing something of ourselves that perhaps we are not able to share with anyone else. Something precious.
And as I walked along a stormy beach today with only sea birds for company, I didn’t just cry, I howled. Because of the something precious that used to sit in the world-space taken up by Carol and by Michelle, and that is now empty. And I didn’t even know it.
But somewhere, also, there is a flicker of gratitude and admiration for the way in which these two women are bringing communities together, even now. The many people at Carol’s funeral, with more people getting ready to travel to London for Michelle’s funeral early next week. The L’Arche London Facebook Messenger group which has over 200 people in it, all over the world, sharing photos and memories of our two friends
And you too, reading these blogs: count yourselves in.
Grieving is hard work. It’s exhausting. We need all the help we can get.
One of the things I’ve always found really helpful is the tradition in our L’Arche community to hold a wake the night before the funeral. It’s often held at the dead person’s home, but in Carol’s case we expected (and got) too large a crowd, so we had the wake in her local church where she was also very much at home. Some people had crossed seas or even oceans to be there.
It’s an opportunity to get together, to think about Carol, to share stories. It’s another opportunity to say goodbye, because her body was there in a small adjacent room, in open coffin, for anyone who wanted to see her one last time.
I went early so I could do just that. I found one of Carol’s dearest friends sitting by the coffin, heartbroken.
“Oh Irene,” she sobbed, and sobbed some more, “I feel such a big part of me has gone.”
I am taken aback by the number of people who feel that a part of them has gone. I was taken aback by my own fresh bout of sobbing, because even though I knew that Carol was dead, seeing her in her coffin brings it home again, just how dead she is.
I spent a long time in that little room. People came and went, all with their own memories, their own way of grieving. Carol’s friends with disabilities were also invited. Some came, some hesitated, some didn’t want to.
Manuela and Serena, Carol’s two housemates who have profound learning disabilities, were among those who came. They needed help to enter, but once in the room they each went uncharacteristically quiet – and then, after what seemed like several minutes of contemplation, each in their own way indicated that it was enough. Manuela wheeled herself out. Serena lost interest in the dead friend and started banging the coffin with great excitement, because that made an lovely noise, so after doing that for a little while, we thought it was time for her to re-join the crowd next door.
I was most deeply touched by Carol’s friend and housemate Peter, who told us last week that he was “hurting in his thoughts”. He came in, clutching his newspaper, and saw Carol in her coffin
“Oh sugar,” he said, once again nailing our feelings exactly.
He stood, and when we suggested he could sit down on one of the few chairs, he sat. What impressed me so much was that this man, who took years (decades, even) to mourn the loss of his mother and could, at first, only express his grief through angry outbursts – could not talk about it for years – was now so at home with his grief for Carol. We were there, but he didn’t really need us, except to give him permission to sit down, to touch the coffin (held held on to it for a very long time), to sit some more.
The one person he did need, and even managed to ask for in this own way, was the priest. “I think Cathy is still around here somewhere,” he kept saying. “I think she’s here.” She was, and she came and sat next to him.
“Carol in my thoughts and up to Jesus Christ,” he said again and again.
Peter is a man of routines. Sitting in a small and quite crowded room, with your dead friend in a coffin, is not part of any routine. But he declined any suggestions that he could leave that little room.
“I think I’ll stay for the second part,” he said, using the language familiar from TV and football.
“Do you mean the second part here in the room with Carol?” one of us asked. Yes, that’s what he meant.
In the church space next door, the slide show had started. Photo after glorious photo, with people chipping in their stories. Ah yes, that was when…. And I remember….
Memories of friendship. Such friendship. But also the memories of how tough things could be, how frustrating and annoying she could be. And the stories that made us laugh.
That time when she had to go into hospital for surgery, and refused the mask for the anaesthetic. Her support assistant started singing “Kung Fu Fighting”, Carol’s favourite song. In the end, the entire crew of theatre staff were belting it out, all in their scrubs. And so, in the end, was Carol, taking a deep in-breath to pitch the killer note – and taking on the mask at the same time.
That time of her very first flight, visiting a friend in Hungary who was getting married. How she stood at the back of the stationary plane, with everyone quietly waiting on the tarmac, shouting at the invisible pilot: “Man! Move!” And the nod of quiet satisfaction when, at last, he did.
“She was bossy!” a young man with Down Syndrome chipped in. “She always bossed Justin around!”
Which prompted David, an longstanding friend of the community, to add: “I often thought Carol had something of the Chicago Underworld about her. That toughness, but with such softness underneath.” We laughed in recognition at this startling new image.
We passed around Carol’s favourite sweets. We sang her favourite songs. We were comforted.
Because we all felt the huge gap Carol leaves behind. Perhaps it is only when someone dies that you really understand their place in the world, and in your life. Indeed, a part of us has gone. As one of Carol’s friends (an assistant who lived with her for several years) said:
So much.
So many memories. Oh, how much I loved her.
Now, I’m donning my hat, and I’m off to Carol’s funeral. See some of you there.
Because it isn’t really about death: it’s about life and about your relationships. So, dying in a way that is as good as possible, whatever that means for you, is hugely important.
It really is a case of all’s well that ends well…
My mission over the past 20 years has been to include everybody, including people with learning disabilities, in all’s well that ends well.
Because if we are not paying attention to how people end their lives, their final months, the final time; and to their deaths and their bereavements – if that doesn’t matter, then what you’re really saying that people’s lives don’t matter.”
That’s what I said in my inaugural lecture last month.
I’ve finally managed to put the film of the lecture on YouTube. Here it is.
I am quite used to giving talks.
It goes with the job. My diary in the next few months includes a masterclass for palliative care professionals in Portugal, a keynote lecture at a conference for cancer nurses in Sweden, a workshop for care staff in learning disability homes in Milton Keynes, and a lecture for MPs, Lords and assorted healthcare professionals at the Houses of Parliament here in London.
But I rarely talk publicly about what I’ve learned in the L’Arche community, where I lived for eight years when I first came to England. It is sometimes hard to explain the bonds of friendship formed in those years of shared living, and how they have shaped my life and my work, even my work as an academic.
Sometimes it’s easy to forget about those bonds.
But at a time like this, when (ex-)L’Arche community members all over the world are coming together to mourn the deaths of Carol and Michelle, when people who haven’t seen each other for years are sharing memories, laughter, tears – I understand afresh why Michelle and Carol are so important in my life.
So it seems quite extraordinary that in my inaugural lecture last month, I did talk about L’Arche, and about friendships, and about bonds. I even had a slide and a story about Michelle. (It starts at 15 mins in the film of the lecture).
I’m glad I did, because now, when friends and colleagues ask me how I am, all I have to say is, Remember Michelle? The woman I shared a room with, who looked after me when I was ill?
She died.
And I don’t have to explain why that matters so much, because it is obvious.
Michelle’s and Carol’s deaths matter because their lives mattered.



































 There was standing room only at
There was standing room only at 





