
Hands up. How many of you readers of this blog have an end-of-life care plan?
Hm. Thought as much. How about a written-down funeral plan?
If your answer was “no”, you’re not alone. When I ask this question in groups of people working in learning disability services, I can usually count the hands on one hand.
If you didn’t raise your hand just now: WHY do you not have an end-of-life care plan handy and waiting in your kitchen drawer? Is it because:
(a) You don’t like to think about death and dying. Let’s pretend we are all immortal.
(b) You are nowhere near the end of your life. You’re fit and well and you’re hoping to live another 30 years. Plenty of time later. No need to get ahead of ourselves.
(c) You have no idea what your end of life will look like, where you’ll be, what you’re going to die of, what your needs will be – so really rather tricky to make a detailed plan.
(d) All of the above.
Let me come clean here: I hadn’t raised my hand either. My reason (if you’re interested) was (c).
I don’t even have a funeral plan. I did in the past (occupational hazard – hospice nurses were sent on courses where you had to visualise your own death and plan for it) but I no longer like the music I liked then, plus I’ve acquired a husband and several children who might want to have a say in the matter. I probably should get a bit more concrete about this though – perhaps the reason for my lack of a funeral plan is a little bit of (b), mixed in with a concern that by the time my 30 years are up, yet another hymn will have become my favourite, so I’d rather not commit to Mozart’s Ave Verum Corpus quite yet.
(Quite fancy the cardboard coffin though. Decorated by my family. Let me put it on the record. Saves me writing it down and sticking it in the kitchen drawer.)
Now, here is the question this is all leading to.
Should ALL people with learning disabilities have an End-of-Life Care plan? Or a Death Plan?
I mean all of them. Young and old. Healthy and ill. Regardless of whether they want one or not.
This question has raised its head repeatedly over the past year. Here is an email I received from the mother of a young man with a learning disability and autism.
What I am concerned about is that the residential home he is living in wants me, his mother, to fill in a form for a “death plan”… The manager said all residents are filling these forms in and it is important to get this in place in the “care plans”. Could you please tell me why there is so much emphasis on this “end of life” stuff, as the majority of these people are still young?
Not surprisingly, both the mother and the son were rather distressed by being asked to plan for death.
Then there are the questions I get from learning disability service providers. Here is an email from someone who works at a large UK-wide organisation. A few of their services had recently been inspected by the CQC. That’s the Care Quality Commission, responsible for regulating and inspecting health and social care services. Inspectors will come round to your care home, look at everything from paperwork to paintwork, talk to anyone from manager to staff to people-who-live-there, and then publish their verdict: Outstanding, Good, Requires improvement, or Inadequate.
The email said:
During the initial feedback, the inspectors have commented about how we haven’t explored end of life with everyone we support and that we haven’t documented their wishes. I feel extremely uncomfortable with these comments – some of the people we support are my age and I would be very insulted/upset/angry if anyone tried to have a discussion with me about what casket I would want if I died.
Another manager I spoke to recently said:
Our service has produced easy-read end of life plans for people. We discussed them in a home where six people with learning disabilities live. Two people wanted to do the plan, but the other four didn’t. When the CQC inspectors came, they marked us down for only having an end of life plan in two people’s files, not all six.
A student learning disability nurse told me a couple of weeks ago:
On one of my placements, ALL residents had an end-of-life plan in their personal files. Put there by the manager, presumably. They all looked identical.
Oh dear. What is going on? It’s no wonder that the most frequent question I get from learning disability services is “Do you have an easy-read end-of-life plan that we can use?”
As it happens, there are plenty of templates around. The PCPLD Network has collated some of them on this page. But I feel uncomfortable with all of them, because of two fundamental problems.
Problem 1: If you standardise personalised care, it is in great danger of becoming impersonal.
If I were an inspector of a home of six people with learning disabilities, and they all had an identical-looking end-of-life plan in their notes, I would hear alarm bells. Documenting someone’s end-of-life wishes should come at the end of a process of discussions and explorations, and it should be regularly reviewed. The format of documentation should fit the person. A document, easy-read or otherwise, is not the starting point. It’s the end point.
Problem 2: Most of these documents are not End of Life Plans. They are Funeral Plans.
Nothing wrong with having a funeral plan, but don’t call it an End of Life Plan. And definitely don’t call it an End of Life Care Plan. The trouble is that I’m not sure what people actually mean when they talk about “end of life care planning”. (And with people, I mean everyone. Families, service providers, inspectors.)
Confusion reigns…
CONFUSION: What is (and what isn’t) an end of life care plan?
What should go in it? When should it be made? Crucial questions. I’ll try and answer them in my next blog post.
CONFUSION: With regard to end of life care and planning for the end of life, what exactly are the CQC requirements?
What is expected of services that provide day-to-day support for people with learning disabilities of all ages (including residential care)? This one was intriguing, so I did a bit of digging. First, I looked up what the CQC inspection criteria actually are. I found that for adult social care services, there is indeed this inspection question (see p.17 of this document): 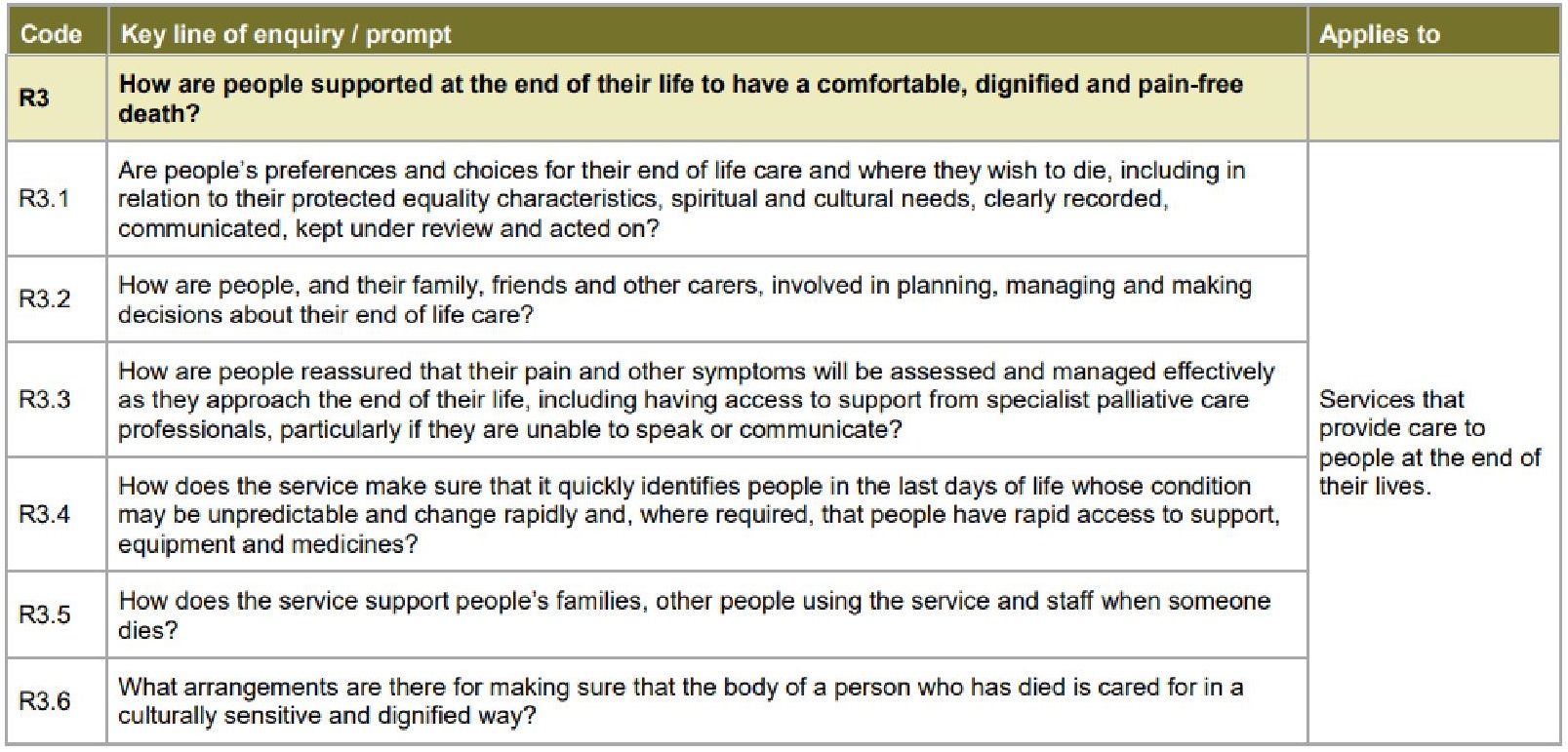
But whilst most other “key lines of enquiry” apply to All Services, this one applies only to Services that provide care to people at the end of their lives.
I searched on. What do they mean by “the end of their lives”? I could not find a description of this anywhere in relation to adult social care services, but this is how “end of life care” is defined in relation to hospital services (and it’s a good definition, used widely):
End of life care involves all care for patients who are approaching the end of their life and following death. (…) The definition of end of life includes patients who are ‘approaching the end of life’ when they are likely to die within the next 12 months. This includes patients whose death is imminent (expected within a few hours or days) and those with:
advanced, progressive, incurable conditions
general frailty and co-existing conditions that mean they are expected to die within 12 months
existing conditions that put them at risk of dying if there is a sudden acute crisis in that condition
life-threatening acute conditions caused by sudden catastrophic events.
The hospital inspection criteria include the following questions: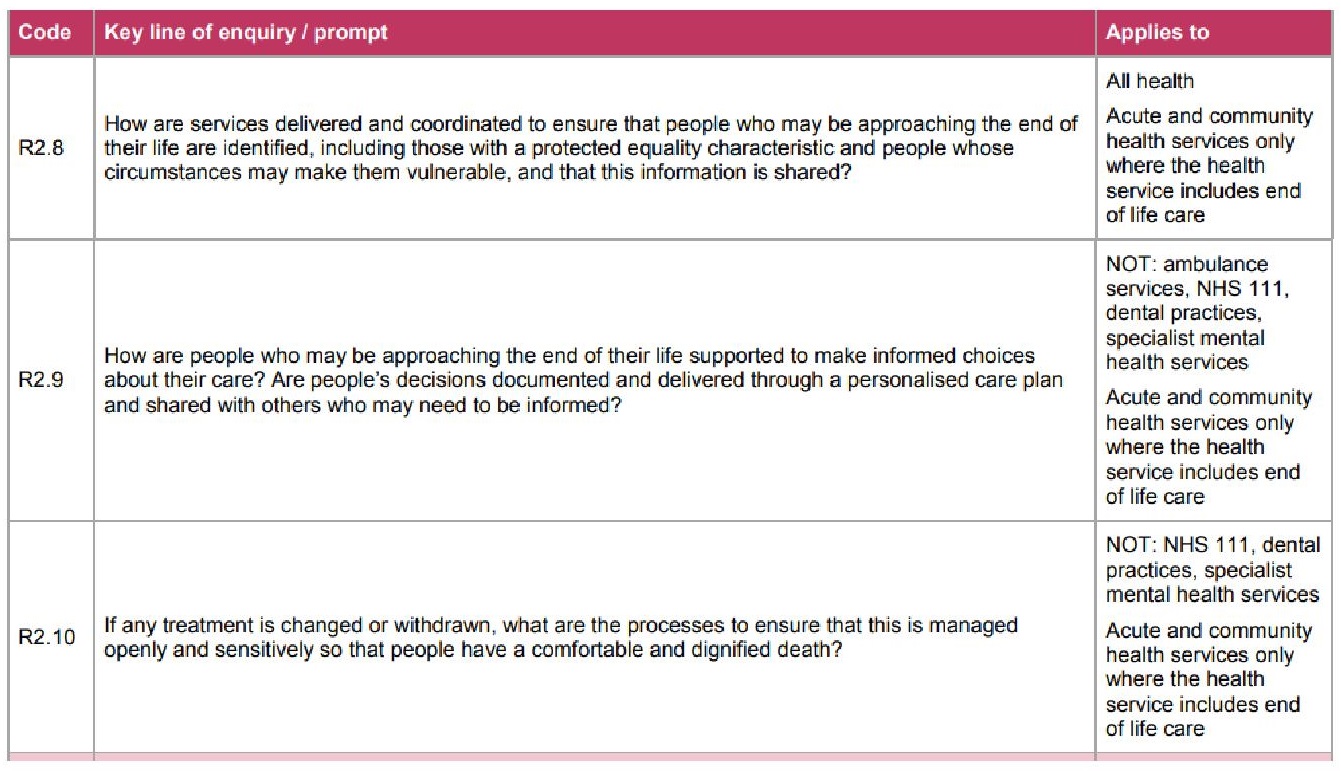
Perhaps the CQC confusion arises from the fact that many learning disabilities aim to provide “homes for life”, so in theory that includes caring for people at the end of their lives. And yes, I agree that all services should know how to spring into action when the people they support do indeed reach the end of their lives. And, as the CQC rightly points out, timely recognition that the end of life is approaching is a sign of outstanding care.
(Quite how you do this is a different question altogether, that would turn this blog post into a book, but I’ll give you the conclusion: “More research is needed.”)
So… does it mean that all people with learning disabilities should have a personalised end-of-life support plan, ready to go? Or only those who are actually approaching the end of life?
I decided to go straight to the horses’ mouth, and got in touch with the Regulatory Manager at the CQC.
Which particular services, exactly, does the R3 requirement apply to? This is what they said (via email, so I’ve got it in writing):
Interpretation of whether R3 applies or not depends then on a combination of inspector judgement and provider positioning – a ‘hard and fast rule’ is counter to CQC’s general approach which focuses on outcomes for people. I would say that in the general course of things, R3 would apply more typically in hospice and palliative care environments rather than general learning disability provision per se.
Does that mean that the CQC inspectors got it wrong? The ones who marked down a service for not having end-of-life care plans for all six residents with learning disabilities? I don’t know enough of the details, but it’s certainly worth debating. This is what my CQC Regulatory Manager went on to say (and I’m quoting a large chunk of email here – the red italics are mine):
I think in summary I would want to say that in my view there is no blanket requirement for providers to have in place an end-of-life plan of care for a person with a learning disability. If such a person is known to be in the end stages of their life, R3 would be engaged in adult social care services, and R2.8-R2.10 in hospital/healthcare CQC registered settings. For staff to discuss a person’s wishes upon their illness or death does not necessarily presuppose the need to have a detailed plan for it. I would agree that there needs to be nuance and personalisation in how these matters might be discussed with people and their families, and that it would not be appropriate or needed in all settings at all times.
They end the email with this invitation (do take them up on it, if you feel the need):
It is open to providers to discuss with CQC during or after the inspection if they think that CQC have misinterpreted the needs of people being met at a particular services.
So there you have it. By all means, talk about death and dying with everyone.
And by all means, if a person with learning disabilities is interested in thinking about their funeral and documenting their wishes, support them. Find a personalised and meaningful way of thinking and talking and documenting this together. Who knows, someone may have strong views on whether they’d like the mourners at their funeral to have tea or coffee.
(Personally, I don’t care, and I wouldn’t wish to document it. What if I specify tea and cakes, but my children are longing for a whiskey and crisps? So I’m a bit puzzled by some of the easy-read “end-of-life plans” I’ve seen that focus on those kind of choices. If I needed to present someone who needs decision-making support with a list of possible choices, their post-funeral refreshments wouldn’t be top of my list. How about helping them choose what refreshments they themselves would like to have right now?)
An end-of-life care plan is something quite different.
It is a dynamic plan that should be put in place for anyone who fits the “approaching the end of life” criteria I described earlier. Of course the difficulty is that death is so unpredictable. Who knows? The best I can give you is what is known as the Surprise Question in palliative care:
Would you be surprised if this person died within the next 12 months?
That person may or may not have a diagnosed terminal illness. But if your answer to the Surprise Question is No, actually, I wouldn’t be that surprises, then it is time to start planning. As they say, “Hoping for the best, preparing for the worst.”
To be continued.
PS Unless I’ve missed something, there is no CQC requirement that All people with learning disabilities must have a funeral plan in their files.
And another PS… In our GRASSroots group of people with learning disabilities, who have been meeting monthly for the past four years to talk about dying, we have an annual vote on what the group would like to do. These two choices have been consistently voted down, so we haven’t done them. Not sure what the moral of that story is.
I really like your sensitive analysis and its helped me put it into perspective. Why do we feel the need to catastrophise a natural process and I love the idea of differentiating between end of life care and a funeral plan.
Pingback: End of life care planning and people with learning disabilities (PART 2) |